

Primary CNS Lymphomas: Challenges in Diagnosis and Monitoring
- PMID: 30035121
- PMCID: PMC6033255
- DOI: 10.1155/2018/3606970
Primary CNS Lymphomas: Challenges in Diagnosis and Monitoring
Abstract
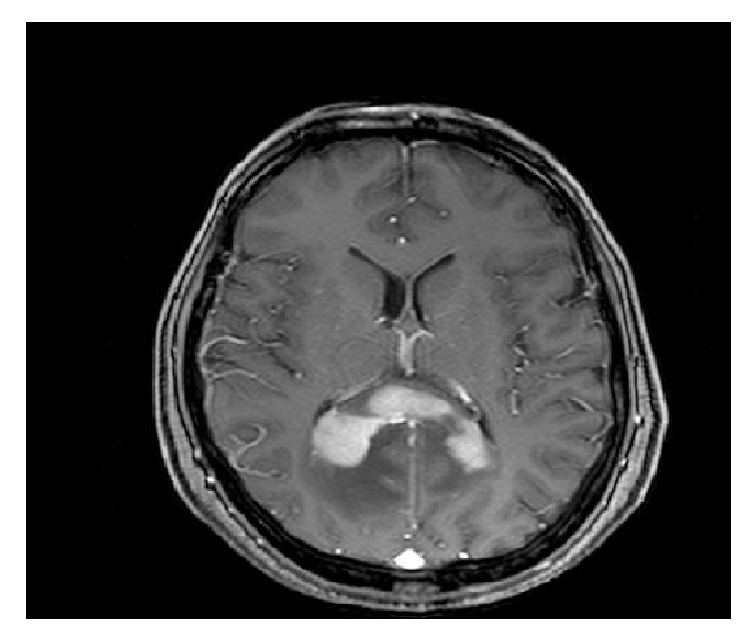
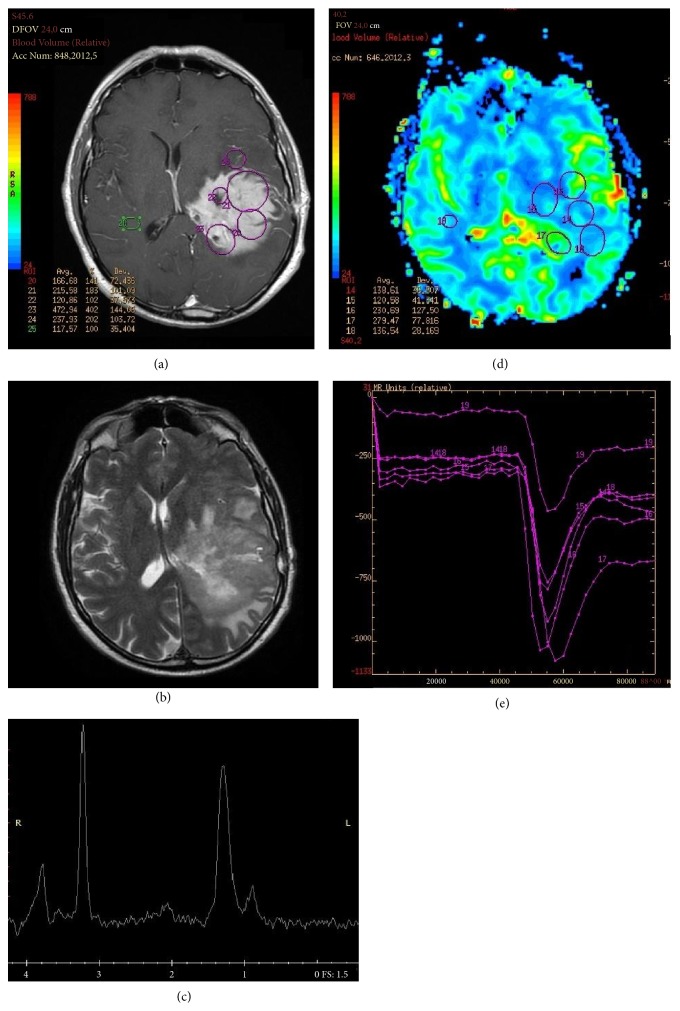
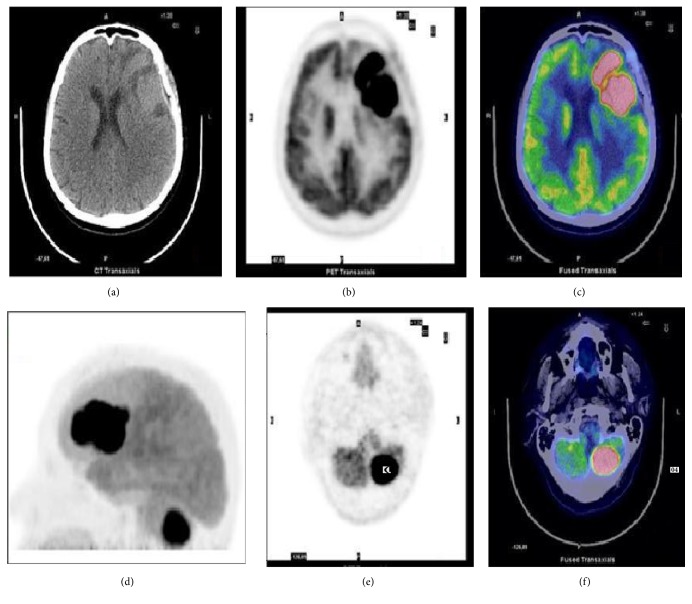
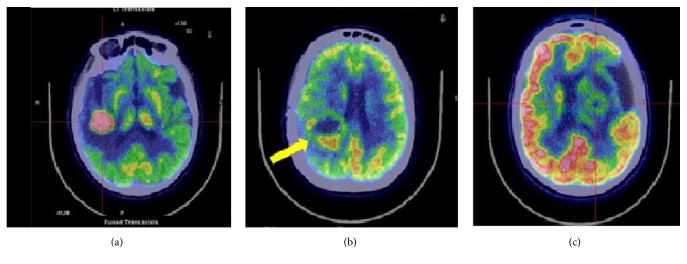
Primary Central Nervous System Lymphoma (PCNSL) is a rare neoplasm that can involve brain, eye, leptomeninges, and rarely spinal cord. PCNSL lesions most typically enhance homogeneously on T1-weighted magnetic resonance imaging (MRI) and appear T2-hypointense, but high variability in MRI features is commonly encountered. Neurological symptoms and MRI findings may mimic high grade gliomas (HGGs), tumefactive demyelinating lesions (TDLs), or infectious and granulomatous diseases. Advanced MRI techniques (MR diffusion, spectroscopy, and perfusion) and metabolic imaging, such as Fluorodeoxyglucose Positron Emission Tomography (FDG-PET) or amino acid PET (usually employing methionine), may be useful in distinguishing these different entities and monitoring the disease course. Moreover, emerging data suggest a role for cerebrospinal fluid (CSF) markers in predicting prognosis and response to treatments. In this review, we will address the challenges in PCNSL diagnosis, assessment of response to treatments, and evaluation of potential neurotoxicity related to chemotherapy and radiotherapy.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
