

Assessment of a renal angina index for prediction of severe acute kidney injury in critically ill children: a multicentre, multinational, prospective observational study
- PMID: 30035208
- PMCID: PMC6053052
- DOI: 10.1016/S2352-4642(17)30181-5
Assessment of a renal angina index for prediction of severe acute kidney injury in critically ill children: a multicentre, multinational, prospective observational study
Abstract
Background: Acute kidney injury (AKI) occurs in one in four children admitted to the intensive care unit (ICU) and AKI severity is independently associated with increased patient morbidity and mortality. Early prediction of AKI has the potential to improve outcomes. In smaller, single center populations, we have previously derived and validated the performance of the renal angina index (RAI), a context driven risk stratification system, to predict severe AKI.
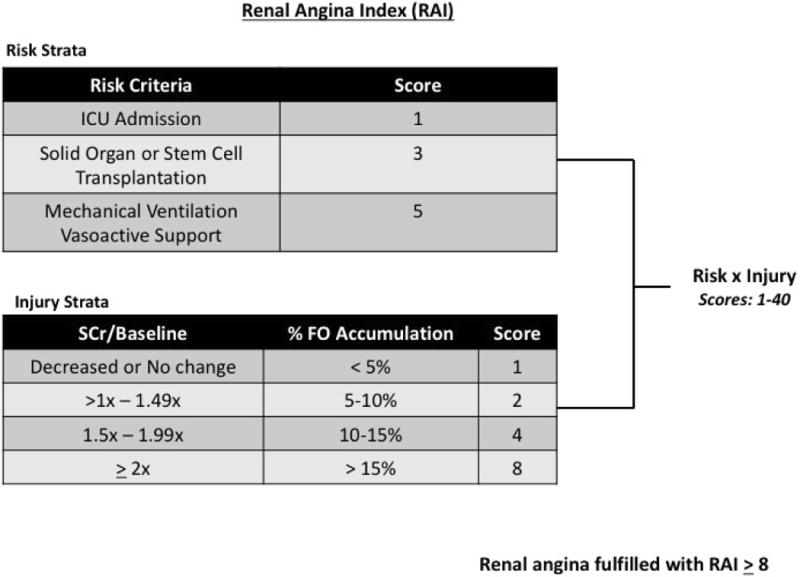
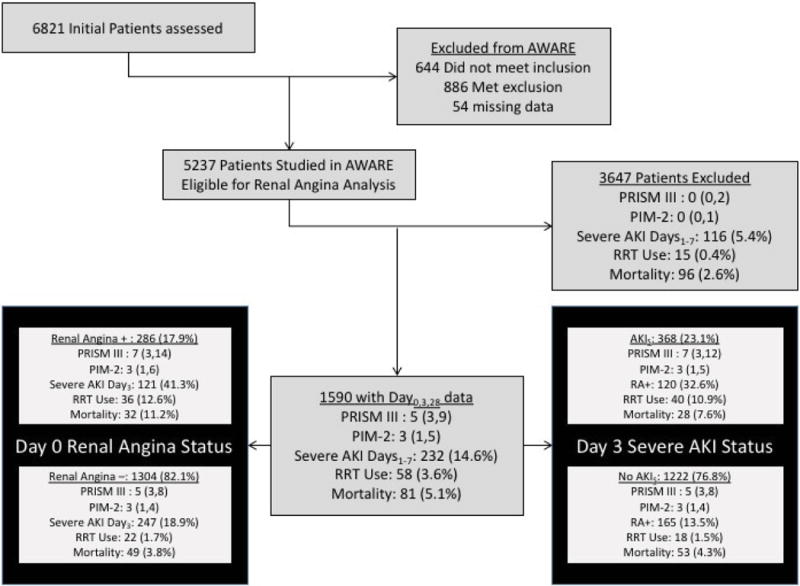
Methods: A prospective, observational study (AWARE1, January-December 2014) was conducted in intensive care units from 32 centers in 9 countries. The primary outcome was the presence of severe AKI ("AKIS"; Stage 2-3 AKI KDIGO guidelines) on the third day after ICU admission (). We compared the performance of the RAI to changes in serum creatinine relative to baseline (SCr/Base) for prediction of the primary outcome and secondary outcomes of interest. A RAI ≥ 8 defined fulfillment of renal angina (RA+); RA+ was compared to SCr increased relative to baseline ("SCr>Base"; using maximum SCr in first 12 hours of ICU admission).
Findings: The 1590 patients studied were 55% male and had median age of 54.5 months. 286 patients (17.9%) were RA+. AKIS occurred in 121 (42.3%) RA+ vs. 247 (18.9%) RA-patients (relative risk (RR) 2.23; 95% confidence interval (CI): 1.87-2.66, p<0.001). 368 (23.1%) patients with AKIS had increased renal replacement therapy utilization (10.9% vs. 1.5%, p<0.001) and increased mortality (7.6% vs. 4.3%, p=0.01) compared to patients without AKIS. RA+ demonstrated better prediction for AKIS than SCr>Base (RR: 1.61; (1.33-1.93), p<0.001) which was maintained on multivariate regression (independent odds ratio (OR): RA+ 3.21; 95% CI (2.20-4.67) vs. SCr>Base 0.68; 95% CI (0.49-4.94)).
Interpretation: Earlier, better prediction of severe AKI has the potential to improve AKI associated patient outcomes. Compared to isolated, context-free changes in SCr, renal angina risk assessment improved accuracy for prediction of severe AKI in critically ill children and young adults.
Conflict of interest statement
Conflict of Interest: none
Figures
Comment in
-
A renal angina index to overcome the silence of the kidneys.Lancet Child Adolesc Health. 2018 Feb;2(2):83-84. doi: 10.1016/S2352-4642(17)30183-9. Epub 2017 Dec 20. Lancet Child Adolesc Health. 2018. PMID: 30169240 No abstract available.
-
Risk of chronic kidney disease after acute kidney injury in critically ill children.Lancet Child Adolesc Health. 2018 Apr;2(4):e4. doi: 10.1016/S2352-4642(18)30065-8. Epub 2018 Mar 13. Lancet Child Adolesc Health. 2018. PMID: 30169302 No abstract available.
References
-
- Hoste EA, Bagshaw SM, Bellomo R, et al. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Intensive care medicine. 2015;41(8):1411–23. - PubMed
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int. 2012;(suppl (2)):1–138.
-
- Rizo-Topete LM, Rosner MH, Ronco C. Acute Kidney Injury Risk Assessment and the Nephrology Rapid Response Team. Blood Purif. 2017;43(1–3):82–8. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical