

Phase I study of dose escalation to dominant intraprostatic lesions using high-dose-rate brachytherapy
- PMID: 30038638
- PMCID: PMC6052382
- DOI: 10.5114/jcb.2018.76881
Phase I study of dose escalation to dominant intraprostatic lesions using high-dose-rate brachytherapy
Abstract
Purpose: Radiation dose escalation for prostate cancer improves biochemical control but is limited by toxicity. Magnetic resonance spectroscopic imaging (MRSI) can define dominant intraprostatic lesions (DIL). This phase I study evaluated dose escalation to MRSI-defined DIL using high-dose-rate (HDR) brachytherapy.
Material and methods: Enrollment was closed early due to low accrual. Ten patients with prostate cancer (T2a-3b, Gleason 6-9, PSA < 20) underwent pre-treatment MRSI, and eight patients had one to three DIL identified. The eight enrolled patients received external beam radiation therapy to 45 Gy and HDR brachytherapy boost to the prostate of 19 Gy in 2 fractions. MRSI images were registered to planning CT images and DIL dose-escalated up to 150% of prescription dose while maintaining normal tissue constraints. The primary endpoint was genitourinary (GU) toxicity.
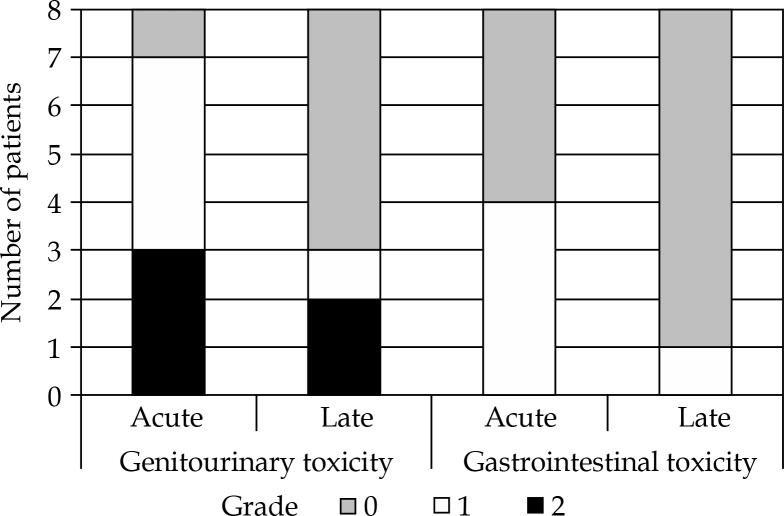
Results: The median total DIL volume was 1.31 ml (range, 0.67-6.33 ml). Median DIL boost was 130% of prescription dose (range, 110-150%). Median urethra V120 was 0.15 ml (range, 0-0.4 ml) and median rectum V75 was 0.74 ml (range, 0.1-1.0 ml). Three patients had acute grade 2 GU toxicity, and two patients had late grade 2 GU toxicity. No patients had grade 2 or higher gastrointestinal toxicity, and no grade 3 or higher toxicities were noted. There were no biochemical failures with median follow-up of 4.9 years (range, 2-8.5 years).
Conclusions: Dose escalation to MRSI-defined DIL is feasible. Toxicity was low but incompletely assessed due to limited patients' enrollment.
Keywords: focal; image-guided brachytherapy; intraprostatic; prostate cancer.
Conflict of interest statement
The authors report no conflict of interest.
Figures



References
-
- Kuban DA, Tucker SL, Dong L, et al. Long-term results of the M.D. Anderson randomized dose-escalation trial for prostate cancer. Int J Radiat Oncol Biol Phys. 2008;70:67–74. - PubMed
-
- Zelefsky MJ, Yamada Y, Fuks Z, et al. Long-term results of conformal radiotherapy for prostate cancer: impact of dose escalation on biochemical tumor control and distant metastases-free survival outcomes. Int J Radiat Oncol Biol Phys. 2008;71:1028–1033. - PubMed
-
- Al-Mamgani A, van Putten WLJ, Heemsbergen WD, et al. Update of Dutch multicenter dose-escalation trial of radiotherapy for localized prostate cancer. Int J Radiat Oncol Biol Phys. 2008;72:980–988. - PubMed
-
- Beckendorf V, Guerif S, Le Prisé E, et al. 70 Gy versus 80 Gy in localized prostate cancer: 5-year results of GETUG 06 randomized trial. Int J Radiat Oncol Biol Phys. 2011;80:1056–1063. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous