

Association Between Midlife Risk Factors and Late-Onset Epilepsy: Results From the Atherosclerosis Risk in Communities Study
- PMID: 30039175
- PMCID: PMC6248112
- DOI: 10.1001/jamaneurol.2018.1935
Association Between Midlife Risk Factors and Late-Onset Epilepsy: Results From the Atherosclerosis Risk in Communities Study
Abstract
Importance: The incidence of epilepsy is higher in older age than at any other period of life. Stroke, dementia, and hypertension are associated with late-onset epilepsy; however, the role of other vascular and lifestyle factors remains unclear.
Objective: To identify midlife vascular and lifestyle risk factors for late-onset epilepsy.
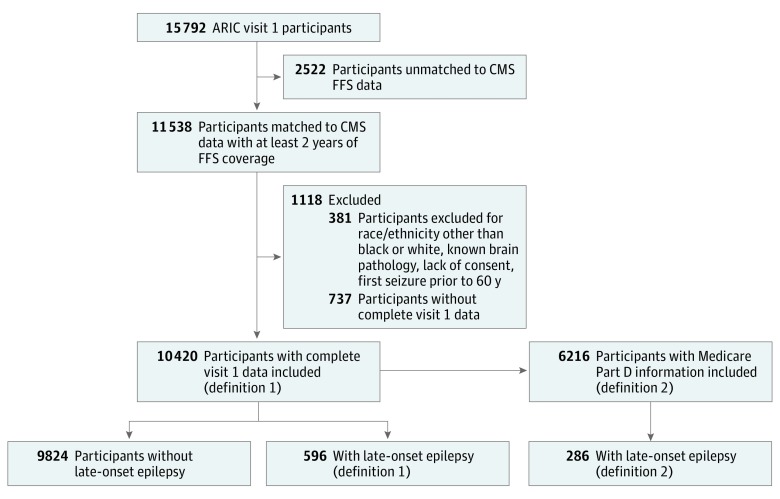
Design, setting, and participants: The Atherosclerosis Risk in Communities (ARIC) study is a prospective cohort study of 15 792 participants followed up since 1987 to 1989 with in-person visits, telephone calls, and surveillance of hospitalizations (10 974 invited without completing enrollment). The ARIC is a multicenter study with participants selected from 4 US communities. This study included 10 420 black or white participants from ARIC with at least 2 years of Medicare fee-for-service coverage and without missing baseline data. Data were analyzed betweeen April 2017 and May 2018.
Exposures: Demographic, vascular, lifestyle, and other possible epilepsy risk factors measured at baseline (age 45-64 years) were evaluated in multivariable survival models including demographics, vascular risk factors, and lifestyle risk factors.
Main outcomes and measures: Time to development of late-onset epilepsy (2 or more International Classification of Diseases, Ninth Revision codes for epilepsy or seizures starting at 60 years or older in any claim [hospitalization or outpatient Medicare through 2013]), with first code for seizures after at least 2 years without code for seizures.
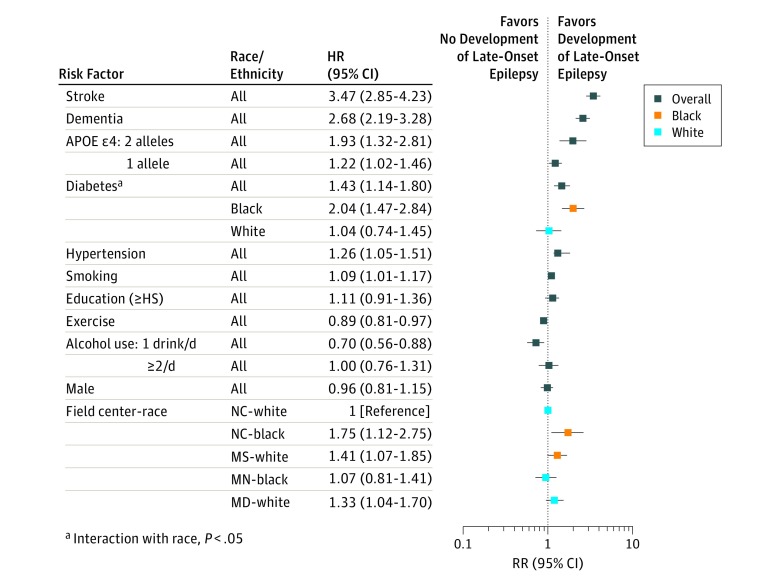
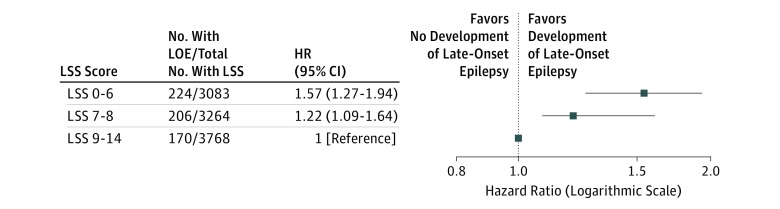
Results: Of the 10 420 total participants (5878 women [56.4%] and 2794 black participants [26.8%]; median age 55 years at first visit), 596 participants developed late-onset epilepsy (3.33 per 1000 person-years). The incidence was higher in black than in white participants (4.71; 95% CI, 4.12-5.40 vs 2.88; 95% CI, 2.60-3.18 per 1000 person-years). In multivariable analysis, baseline hypertension (hazard ratio [HR], 1.30; 95% CI, 1.09-1.55), diabetes (HR, 1.45; 95% CI, 1.17-1.80), smoking (HR, 1.09; 95% CI, 1.01-1.17), apolipoprotein E ε4 genotype (1 allele HR, 1.22; 95% CI, 1.02-1.45; 2 alleles HR, 1.95; 95% CI, 1.35-2.81), and incident stroke (HR, 3.38; 95% CI, 2.78-4.10) and dementia (HR, 2.56; 95% CI, 2.11-3.12) were associated with an increased risk of late-onset epilepsy, while higher levels of physical activity (HR, 0.90; 95% CI, 0.83-0.98) and moderate alcohol intake (HR, 0.72; 95% CI, 0.57-0.90) were associated with a lower risk. Results were similar after censoring individuals with stroke or dementia.
Conclusions and relevance: Potentially modifiable risk factors in midlife and the APOE ε4 genotype were positively associated with risk of developing late-onset epilepsy. Although stroke and dementia were both associated with late-onset epilepsy, vascular and lifestyle risk factors were significant even in the absence of stroke or dementia.
Conflict of interest statement
Figures
Comment in
-
Seize the Day for a Day With No Seizures: Modifiable Midlife Risk Factors Identified.Epilepsy Curr. 2019 Jan;19(1):27-28. doi: 10.1177/1535759718822041. Epub 2019 Jan 30. Epilepsy Curr. 2019. PMID: 30838917 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- U01 HL096812/HL/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- U01 HL096917/HL/NHLBI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- U01 HL096902/HL/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- U01 HL096899/HL/NHLBI NIH HHS/United States
- K24 AG052573/AG/NIA NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
