

Kidney Function, Polypharmacy, and Potentially Inappropriate Medication Use in a Community-Based Cohort of Older Adults
- PMID: 30039344
- PMCID: PMC6093216
- DOI: 10.1007/s40266-018-0563-1
Kidney Function, Polypharmacy, and Potentially Inappropriate Medication Use in a Community-Based Cohort of Older Adults
Abstract
Background: Chronic kidney disease (CKD) afflicts many older adults and increases the risk for medication-related adverse events.
Objective: The aim of this study was to assess the prevalence and associated morbidity and mortality of polypharmacy (use of several medications concurrently), and potentially inappropriate medication (PIM) use in older adults, looking for differences by CKD status.
Methods: We quantified medication and PIM use (from Beers criteria, the Screening Tool of Older People's Prescriptions, and Micromedex®) by level of estimated glomerular filtration rate (eGFR) for participants aged 65 years or older attending a baseline study visit in the Atherosclerosis Risk in Communities study (n =6392). We used zero-inflated negative binomial and Cox proportional hazards regressions to assess the relationship between baseline polypharmacy, PIM use, and subsequent hospitalization and death.
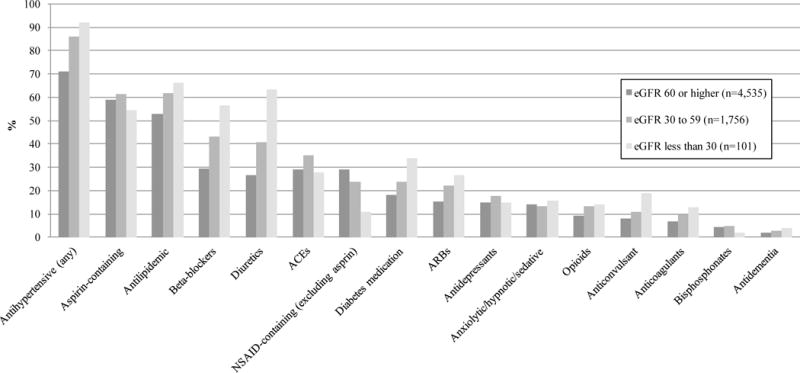
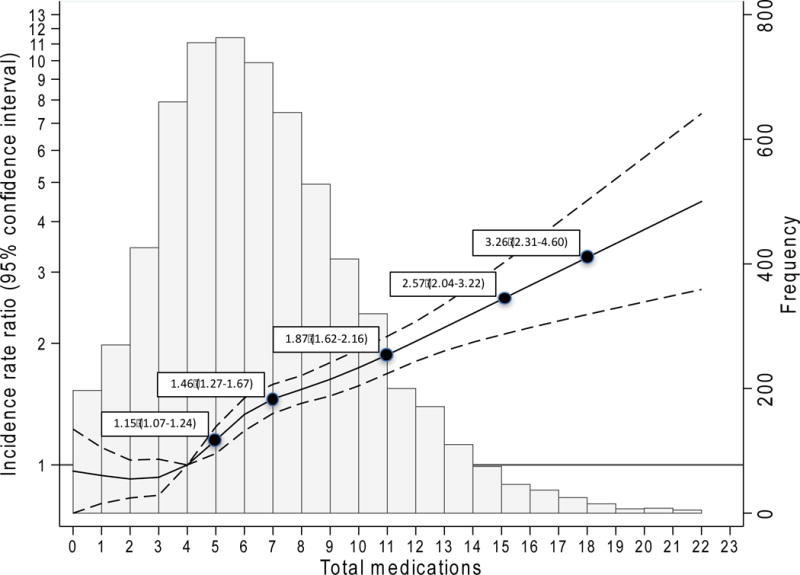
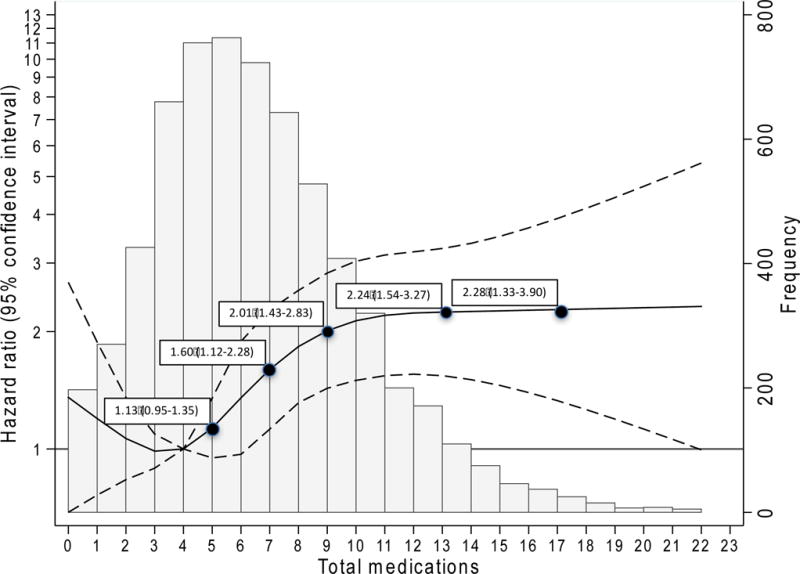
Results: Mean age at baseline was 76 (± 5) years, 59% were female, and 29% had CKD (eGFR < 60 ml/min/1.73 m2). Overall, participants reported 6.1 (± 3.5) medications and 2.3 (± 2.2) vitamins/supplements; 16% reported ≥ 10 medications; 31% reported a PIM based on their age. On average, participants with CKD reported more medications. A PIM based on kidney function was used by 36% of those with eGFR < 30 ml/min/1.73 m2. Over a median of 2.6 years, more concurrent medications were associated with higher risk of hospitalization and death, but PIM use was not. While those with CKD had higher absolute risks, there was no difference in the relative risks associated with greater numbers of medications by CKD status.
Conclusion: Polypharmacy and PIM use were common, with greater numbers of medications associated with higher risk of hospitalization and death; relative risks were similar for those with and without CKD.
Conflict of interest statement
Dr. Alexander is Chair of FDA’s Peripheral and Central Nervous System Advisory, Committee, has served as a paid advisor to IQVIA, serves on the advisory board of, MesaRx Innovations, is a member of OptumRx’s National P&T Committee; and holds, equity in Monument Analytics, a health care consultancy whose clients include the life, sciences industry as well as plaintiffs in opioid litigation. This arrangement has been reviewed and approved by Johns Hopkins University in accordance with its conflict of interest policies. Alex Secora, G. Caleb Alexander, Shoshana Ballew, Josef Coresh and Morgan Grams declare that they have no conflicts of interest relevant to the content of, this study.
Figures
References
-
- He W, Goodkind D, Kowal P. An aging world: 2015 international population reports. Washington, D.C: U.S. Government Publishing Office; Mar, 2016.
-
- Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, et al. Prevalence of chronic kidney disease in the United States. JAMA. 2007;298(17):2038–47. - PubMed
-
- Lassiter J, Bennett WM, Olyaei AJ. Drug dosing in elderly patients with chronic kidney disease. Clin Geriatr Med. 2013;29(3):657–705. - PubMed
-
- Masoudi FA, Baillie CA, Wang Y, Bradford WD, Steiner JF, Havranek EP, et al. The complexity and cost of drug regimens of older patients hospitalized with heart failure in the United States, 1998-2001. Arch Intern Med. 2005;165(18):2069–76. - PubMed
Publication types
MeSH terms
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- U01 FD004977/FD/FDA HHS/United States
- HHSN268201000011C/HL/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- HHSN268201000010C/HL/NHLBI NIH HHS/United States
- K08 DK092287/DK/NIDDK NIH HHS/United States
- T32 HL007024/HL/NHLBI NIH HHS/United States
- HHSN268201000012C/HL/NHLBI NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
