

Early versus delayed antiretroviral treatment in HIV-positive people with cryptococcal meningitis
- PMID: 30039850
- PMCID: PMC6513637
- DOI: 10.1002/14651858.CD009012.pub3
Early versus delayed antiretroviral treatment in HIV-positive people with cryptococcal meningitis
Abstract
Background: There remains uncertainty about the optimum timing of antiretroviral therapy (ART) initiation in HIV-positive people with cryptococcal meningitis. This uncertainty is the result of conflicting data on the mortality risk and occurrence of immune reconstitution inflammatory syndrome (IRIS) when ART is initiated less than four weeks after cryptococcal meningitis treatment is commenced.
Objectives: To compare the outcomes of early initiation of ART (less than four weeks after starting antifungal treatment) versus delayed initiation of ART (four weeks or more after starting antifungal treatment) in HIV-positive people with concurrent cryptococcal meningitis.
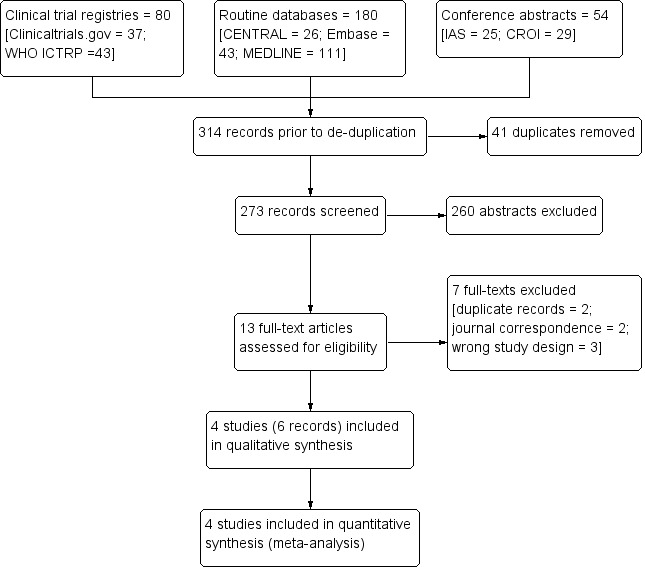
Search methods: We searched the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, and Embase for trials published between 1 January 1980 and 7 August 2017. We additionally searched international trial registries, including ClinicalTrials.gov and WHO International Clinical Trials Registry Platform (ICTRP), and conference abstracts from the International AIDS Society (IAS) and the Conference on Retroviruses and Opportunistic Infections (CROI) for ongoing or unpublished studies between 2015 and 2017. We reviewed reference lists of included studies to identify additional studies.
Selection criteria: We included randomized controlled trials (RCTs) that compared early versus delayed ART initiation in HIV-positive people with cryptococcal meningitis. Children, adults, and adolescents from any setting were eligible for inclusion.
Data collection and analysis: Two review authors independently applied the inclusion criteria and extracted data. We presented dichotomous outcomes as risk ratios (RR) with 95% confidence intervals (CIs). We presented time-to-death data as hazard ratios with 95% CIs. We assessed the certainty of the evidence using the GRADE approach.
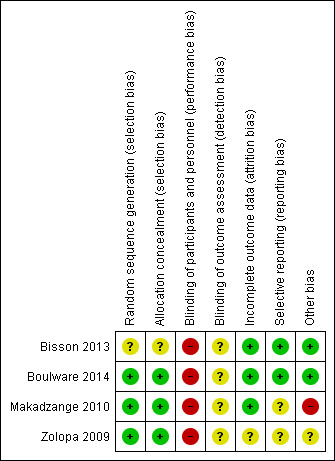
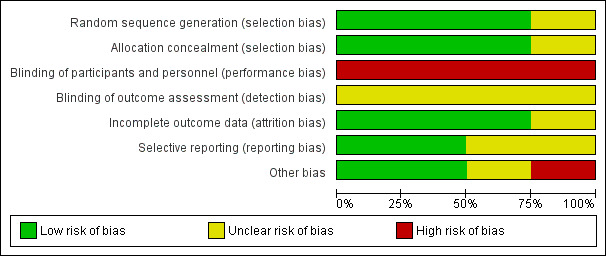
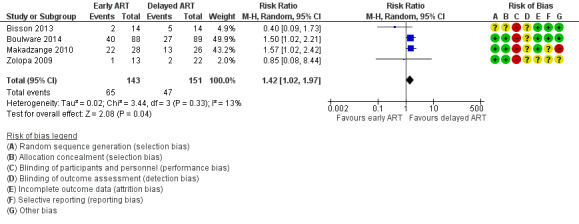
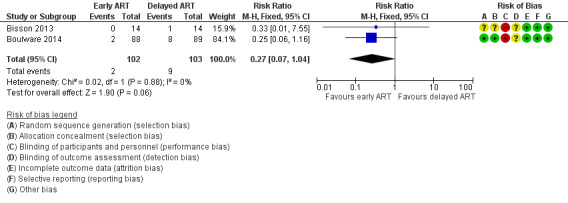
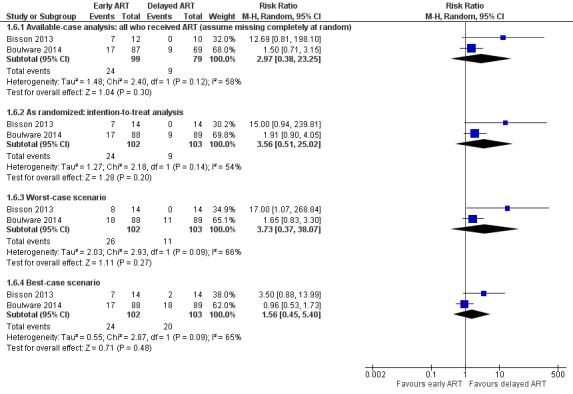
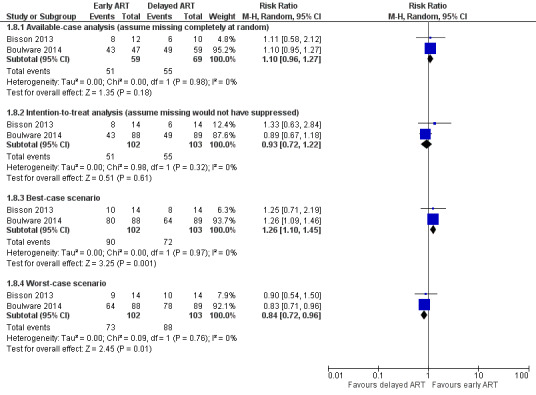
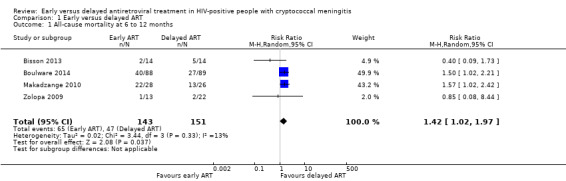
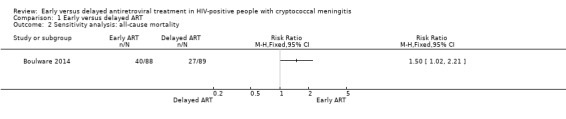
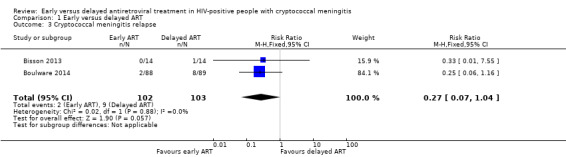
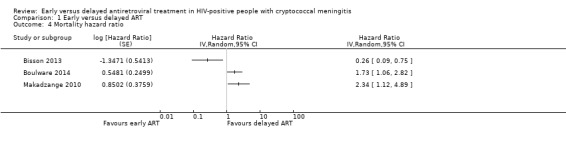
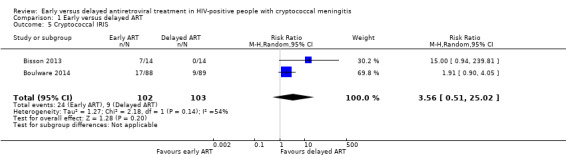
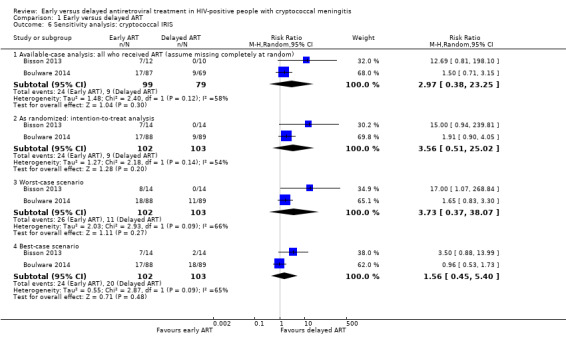
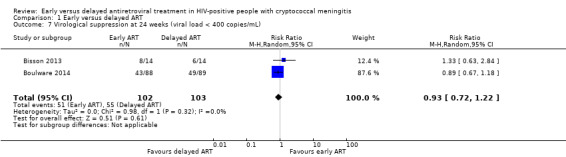
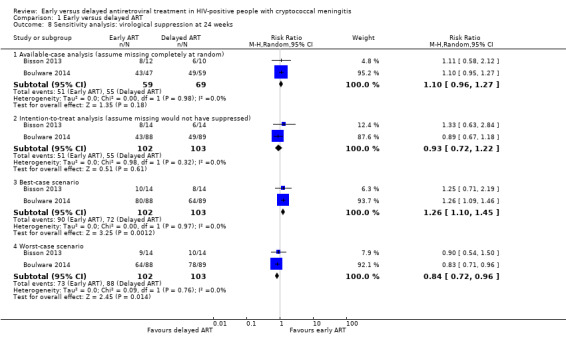
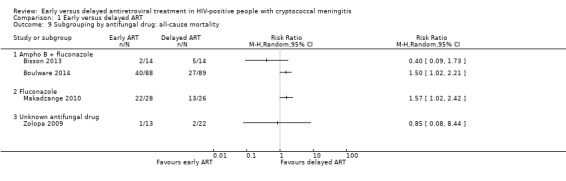
Main results: Four trials including 294 adult participants met the inclusion criteria of this review. Participants were predominantly from low- and middle-income countries. Two trials treated cryptococcal meningitis with amphotericin B and fluconazole; a third trial used fluconazole monotherapy; and the fourth trial did not specify the antifungal used.Early ART initiation may increase all-cause mortality compared to delayed ART initiation (RR 1.42, 95% CI 1.02 to 1.97; 294 participants, 4 trials; low-certainty evidence). Early ART initiation may reduce relapse of cryptococcal meningitis compared to delayed ART initiation (RR 0.27, 95% CI 0.07 to 1.04; 205 participants, 2 trials, low-certainty evidence). We are uncertain whether early ART initiation increases or reduces cryptococcal IRIS events compared to delayed ART initiation (RR 3.56, 95% CI 0.51 to 25.02; 205 participants, 2 trials; I2 = 54%; very low-certainty evidence). We are uncertain if early ART initiation increases or reduces virological suppression at six months compared to delayed ART initiation (RR 0.93, 95% CI 0.72 to 1.22; 205 participants, 2 trials; I2 statistic = 0%; very low-certainty evidence).We were unable to pool results related to rate of fungal clearance for the two trials that reported this outcome; individual trial results indicated that there was no difference in cerebrospinal fluid fungal clearance between trial arms. Similarly, we were unable to pool results on adverse events for the trials reporting on this outcome; individual trial results indicated no difference in the occurrence of grade 3 to 5 adverse events between trial arms.Three of the four included trials had an overall low or unclear risk of bias related to the primary outcome of all-cause mortality. However, we assessed one trial as at high risk of bias due to selective outcome reporting and other bias. This, in addition to the few clinical events and imprecision of effect estimates, led to downgrading of the evidence to low or very low certainty.
Authors' conclusions: The results of this review are relevant to HIV-positive adults with cryptococcal meningitis in low- and middle-income countries. These data suggest a higher risk of mortality among people who initiate ART within four weeks of cryptococcal meningitis diagnosis. However, it is unclear if this higher mortality risk is related to cryptococcal meningitis-IRIS.
Conflict of interest statement
Ingrid Eshun‐Wilson has no known conflicts of interest. Mbah P Okwen has no known conflicts of interest. Marty Richardson has no known conflicts of interest. Tihana Bicanic has received payment of fees and a grant from Gilead and Basilea for advisory board, speaker fees, and grants outside the submitted work.
Figures

Update of
-
Optimal timing for antiretroviral therapy initiation in patients with HIV infection and concurrent cryptococcal meningitis.Cochrane Database Syst Rev. 2013 Feb 28;(2):CD009012. doi: 10.1002/14651858.CD009012.pub2. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2018 Jul 24;7:CD009012. doi: 10.1002/14651858.CD009012.pub3. PMID: 23450595 Updated.
References
References to studies included in this review
Bisson 2013 {published data only}
-
- Bisson GP, Molefi M, Bellamy S, Thakur R, Steenhoff A, Tamuhla N, et al. Early versus delayed antiretroviral therapy and cerebrospinal fluid fungal clearance in adults with HIV and cryptococcal meningitis. Clinical Infectious Diseases 2013;56(8):1165‐73. [DOI: 10.1093/cid/cit019; CN‐00861211] - DOI - PubMed
Boulware 2014 {published data only}
Makadzange 2010 {published and unpublished data}
-
- Makadzange AT, Ndhlovu CE, Takarinda K, Reid M, Kurangwa M, Gona P, et al. Early versus delayed initiation of antiretroviral therapy for concurrent HIV infection and cryptococcal meningitis in sub‐Saharan Africa. Clinical Infectious Diseases 2010;50(11):1532‐8. [DOI: 10.1086/652652; CN‐00748368] - DOI - PubMed
Zolopa 2009 {published data only}
-
- Zolopa A, Andersen J, Powderly W, Sanchez A, Sanne I, Suckow C, et al. Early antiretroviral therapy reduces AIDS progression/death in individuals with acute opportunistic infections: a multicenter randomized strategy trial. PLoS ONE 2009;4(5):e5575. [DOI: 10.1371/journal.pone.0005575; CN‐00702077] - DOI - PMC - PubMed
References to studies excluded from this review
Makadzange 2015a {published data only}
-
- Makadzange AT, Mothobi N. Randomised controlled trial: delaying initiation of ART for 5 weeks improves survival in patients with HIV infection with cryptococcal meningitis. Evidence‐Based Medicine 2015;20(1):15. - PubMed
Makadzange 2015b {published data only}
-
- Makadzange AT, Mothobi N. Delaying initiation of ART for 5 weeks improves survival in patients with HIV infection with cryptococcal meningitis. Evidence‐Based Medicine 2015;20(1):15. - PubMed
Makadzange 2015c {published data only}
-
- Makadzange AT, Mothobi N, Isaac ML, Larson EB, Boulware DR, Meya DB, et al. Delaying initiation of ART for 5 weeks improves survival in patients with HIV infection with cryptococcal meningitis. Evidence‐Based Medicine 2015;20(1):15. - PubMed
Manosuthi 2008 {published data only}
-
- Manosuthi W, Chottanapund S, Sungkanuparph S. Mortality rate of early versus deferred initiation of antiretroviral therapy in HIV‐1‐infected patients with cryptococcal meningitis. Journal of Acquired Immune Deficiency Syndromes 2008;48(4):508‐9. - PubMed
Sungkanuparph 2009 {published data only}
-
- Sungkanuparph S, Filler SG, Chetchotisakd P, Pappas PG, Nolen TL, Manosuthi W, et al. Cryptococcal immune reconstitution inflammatory syndrome after antiretroviral therapy in AIDS patients with cryptococcal meningitis: a prospective multicenter study. Clinical Infectious Diseases 2009;49(6):931‐4. - PubMed
Sunpath 2012 {published data only}
Torok 2005 {published data only}
-
- Torok ME, Day JN, Hien TT, Farrar JJ. Immediate or deferred antiretroviral therapy for central nervous system opportunistic infections?. AIDS 2005;19(5):535‐6. - PubMed
Additional references
Bicanic 2005
-
- Bicanic T, Harrison TS. Cryptococcal meningitis. British Medical Bulletin 2005;72:99‐118. - PubMed
Bicanic 2006
-
- Bicanic T, Harrison T, Niepieklo A, Dyakopu N, Meintjes G. Symptomatic relapse of HIV‐associated cryptococcal meningitis after initial fluconazole monotherapy: the role of fluconazole resistance and immune reconstitution. Clinical Infectious Diseases 2006;43(8):1069‐73. - PubMed
Bicanic 2009
-
- Bicanic T, Meintjes G, Rebe K, Williams A, Loyse A, Wood R, et al. Immune reconstitution inflammatory syndrome in HIV‐associated cryptococcal meningitis: a prospective study. Journal of Acquired Immune Deficiency Syndromes 2009;51(2):130‐4. - PubMed
Bicanic 2010
-
- Bicanic T, Jarvis JN, Muzoora C, Harrison TS. Should antiretroviral therapy be delayed for 10 weeks for patients treated with fluconazole for cryptococcal meningitis?. Clinical Infectious Diseases 2010;51(8):986‐7. - PubMed
Bicanic 2015
-
- Bicanic T, Bottomley C, Loyse A, Brouwer AE, Muzoora C, Taseera K, et al. Toxicity of amphotericin B deoxycholate‐based induction therapy in patients with HIV‐associated cryptococcal meningitis. Antimicrobial Agents and Chemotherapy 2015;59(12):7224‐31. [DOI: 10.1128/AAC.01698-15] - DOI - PMC - PubMed
Boulware 2010
Crabtree Ramírez 2017
GRADEpro GDT 2015 [Computer program]
-
- McMaster University (developed by Evidence Prime, Inc.). GRADEpro GDT. Version accessed 16 July 2017. Hamilton (ON): McMaster University (developed by Evidence Prime, Inc.), 2015.
Grant 2010
-
- Grant PM, Aberg JA, Zolopa AR. Concerns regarding a randomized study of the timing of antiretroviral therapy in Zimbabweans with AIDS and acute cryptococcal meningitis. Clinical Infectious Diseases 2010;51(8):984‐5. - PubMed
Guyatt 2008
Guyatt 2011
Haddow 2010
Higgins 2011
-
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org. Available from handbook.cochrane.org: The Cochrane Collaboration.
Higgins 2016
-
- Higgins JPT, Lasserson T, Chandler J, Tovey D, Churchill R. Standards for the conduct of new Cochrane Intervention Reviews. In: Higgins JPT, Lasserson T, Chandler J, Tovey D, Churchill R. Methodological Expectations of Cochrane Intervention Reviews. London: The Cochrane Library, 2016.
Ingle 2015
-
- Ingle SM, Miro JM, Furrer H, Justice A, Saag MS, Manzardo C, et al. Impact of ART on mortality in cryptococcal meningitis patients: high‐income settings. Conference on Retroviruses and Opportunistic Infections (CROI); 2015 Feb 23‐25; Seattle (WA). San Francisco: CROI Foundation/IAS‐USA, 2015:Poster 837.
Loyse 2013
Lundgern 2015
Meiring 2016
-
- Meiring S, Fortuin‐de Smidt M, Kularatne R, Dawood H, Govender NP, GERMS‐SA. Prevalence and hospital management of amphotericin B deoxycholate‐related toxicities during treatment of HIV‐associated cryptococcal meningitis in South Africa. PLoS Neglected Tropical Diseases 2016;10(7):e0004865. [DOI: 10.1371/journal.pntd.0004865] - DOI - PMC - PubMed
Mwaba 2001
-
- Mwaba P, Mwansa J, Chintu C, Pobee J, Scarborough M, Portsmouth S, et al. Clinical presentation, natural history, and cumulative death rates of 230 adults with primary cryptococcal meningitis in Zambian AIDS patients treated under local conditions. Postgraduate Medical Journal 2001;77(914):769–73. - PMC - PubMed
Müller 2010
-
- Müller M, Wandel S, Colebunders R, Attia S, Furrer H, Egger M, IeDEA Southern, Central Africa. Immune reconstitution inflammatory syndrome in patients starting antiretroviral therapy for HIV infection: a systematic review and meta‐analysis. Lancet Infectious Diseases 2010;10(4):251‐61. - PMC - PubMed
NIH 2017a
-
- AIDSinfo. Guidelines for the prevention and treatment of opportunistic infections in HIV‐infected adults and adolescents: recommendations from the Centers for Disease Control and Prevention, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. aidsinfo.nih.gov/contentfiles/lvguidelines/adult_oi.pdf (accessed prior to 13 September 2017).
NIH 2017b
-
- AIDSinfo. Guidelines for the prevention and treatment of opportunistic infections among HIV‐exposed and HIV‐infected children. https://aidsinfo.nih.gov/guidelines/html/4/adult‐and‐adolescent‐opportun... (accessed prior to 29 September 2017).
Park 2009
-
- Park BJ, Wannemuehler KA, Marston BJ, Govender N, Pappas PG, Chiller TM. Estimation of the current global burden of cryptococcal meningitis among persons living with HIV/AIDS. AIDS 2009;23(4):525‐30. - PubMed
Rajasingham 2017
RevMan 2014 [Computer program]
-
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Shelburne 2005
-
- Shelburne SA 3rd, Darcourt J, White AC Jr, Greenberg SB, Hamill RJ, Atmar RL, et al. The role of immune reconstitution inflammatory syndrome in AIDS‐related Cryptococcus neoformans disease in the era of highly active antiretroviral therapy. Clinical Infectious Diseases 2005;40(7):1049‐52. - PubMed
Tinashe 2016
UNAIDS 2017
-
- Joint United Nations Programme on HIV/AIDS (UNAIDS). UNAIDS global AIDS update. www.unaids.org/sites/default/files/media_asset/20170720_Data_book_2017_e... (accessed prior to 1 September 2017).
WHO 2013
-
- World Health Organization. HIV/AIDS: prevention screening and management of common coinfections. Consolidated ARV guidelines, June 2013. www.who.int/hiv/pub/guidelines/arv2013/coinfection/prevcoinfection/en/in... (accessed prior to 31 June 2017).
WHO 2016
-
- World Health Organization. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. Recommendations for a public health approach. Second edition. www.who.int/hiv/pub/arv/arv‐2016/en/ (accessed prior to 13 September 2017).
WHO 2018
-
- World Health Organization. Guidelines for the diagnosis, prevention and management of cryptococcal disease in HIV‐infected adults, adolescents and children. Supplement to the 2016 consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. www.who.int/hiv/pub/guidelines/cryptococcal‐disease/en/ (accessed prior to 25 April 2018). - PubMed
Williamson 2017
-
- Williamson PR, Jarvis JN, Panackal AA, Fisher MC, Molloy SF, Loyse A, et al. Cryptococcal meningitis: epidemiology, immunology, diagnosis and therapy. Nature Reviews Neurology 2017;13(1):13‐24. - PubMed
References to other published versions of this review
Njei 2011
Njei 2013
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous