

Evidence-based usability design principles for medication alerting systems
- PMID: 30041647
- PMCID: PMC6057098
- DOI: 10.1186/s12911-018-0615-9
Evidence-based usability design principles for medication alerting systems
Abstract
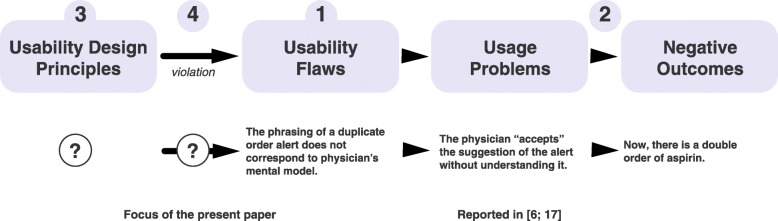
Background: Usability flaws in medication alerting systems may have a negative impact on clinical use and patient safety. In order to prevent the release of alerting systems that contain such flaws, it is necessary to provide designers and evaluators with evidence-based usability design principles. The objective of the present study was to develop a comprehensive, structured list of evidence-based usability design principles for medication alerting systems.
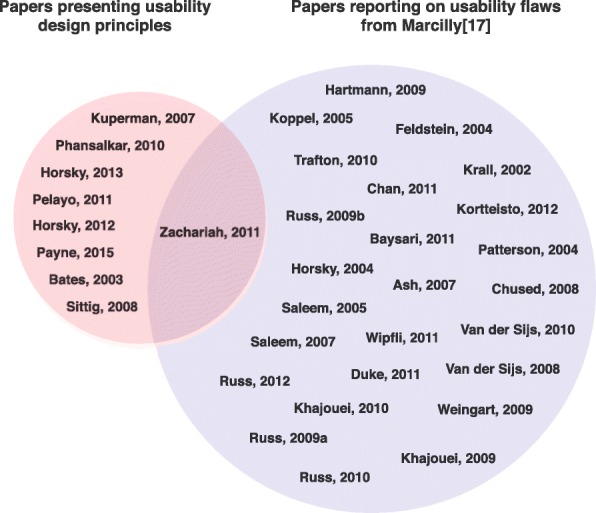
Methods: Nine sets of design principles for medication alerting systems were analyzed, summarized, and structured. We then matched the summarized principles with a list of usability flaws in order to determine the level of underlying evidence.
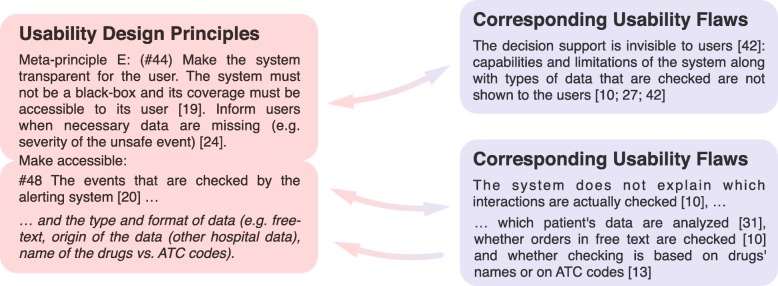
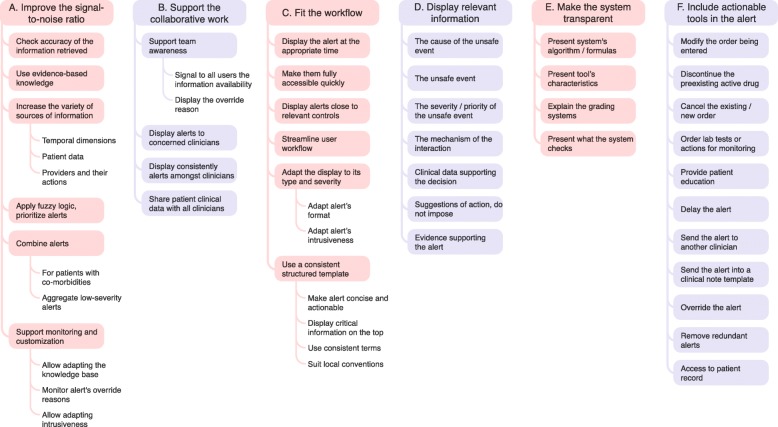
Results: Fifty-eight principles were summarized from the literature and two additional principles were defined, so that each flaw was matched with a principle. We organized the 60 summarized usability design principles into 6 meta-principles, 38 principles, and 16 sub-principles. Only 15 principles were not matched with a usability flaw. The 6 meta-principles respectively covered the improvement of the signal-to-noise ratio, the support for collaborative working, the fit with a clinician's workflow, the data display, the transparency of the alerting system, and the actionable tools to be provided within an alert.
Conclusions: It is possible to develop an evidence-based, structured, comprehensive list of usability design principles that are specific to medication alerting systems and are illustrated by the corresponding usability flaws. This list represents an improvement over the current literature. Each principle is now associated with the best available evidence of its violation. This knowledge may help to improve the usability of medication alerting systems and, ultimately, decrease the harmful consequences of the systems' usability flaws.
Keywords: Alerting system; Decision support; Design; Human engineering; Usability.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Bates DW, Kuperman GJ, Wang S, Gandhi T, Kittler A, Volk L, Spurr C, Khorasani R, Tanasijevic M, Middleton B. Ten commendments for effective clinical decision support: making the practice of evidence-based medicine a reality. J Am Med Inform Assoc. 2003;10:523–530. doi: 10.1197/jamia.M1370. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
