

Gene therapy in hemophilia A: a cost-effectiveness analysis
- PMID: 30042145
- PMCID: PMC6058236
- DOI: 10.1182/bloodadvances.2018021345
Gene therapy in hemophilia A: a cost-effectiveness analysis
Abstract
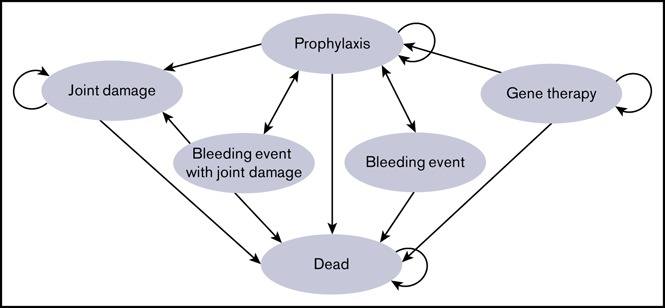
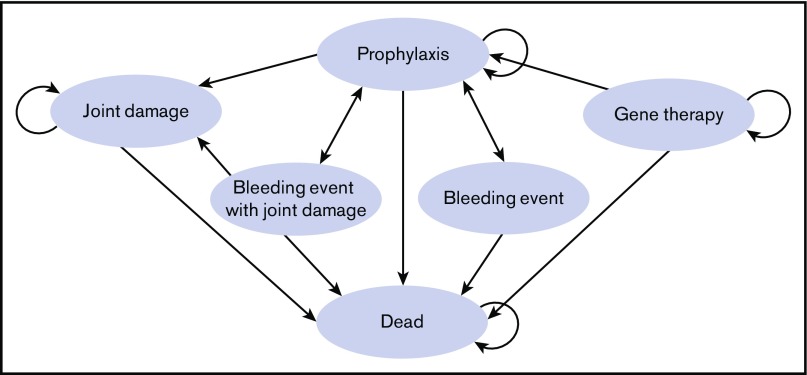
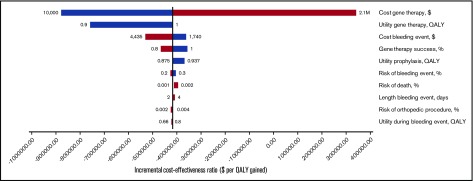
Gene therapy provides a potential phenotypic cure for hemophilia, yet the cost of this novel treatment is high, tempering enthusiasm and raising questions regarding cost vs benefit. To evaluate the cost-effectiveness of gene therapy treatment of severe hemophilia A compared with prophylaxis with factor VIII (FVIII), we developed a Markov state-transition model to estimate the costs and effectiveness of severe hemophilia A treatment strategies from a United States health care system perspective. Quality-adjusted life-years (QALYs) were the effectiveness measure. In the base case, hypothetical cohorts of 30-year-old patients received gene therapy or FVIII prophylaxis. We obtained model probabilities and utilities from the literature and costs from Medicare reimbursement data. One-way and probabilistic sensitivity analyses were performed to test the robustness of results. Over a 10-year time horizon, total per-person gene therapy strategy costs were $1.0M and resulted in 8.33 QALYs, whereas prophylaxis cost $1.7M and resulted in 6.62 QALYs. Thus, gene therapy dominated prophylaxis (costs less and was more effective). Gene therapy remained dominant unless initial costs exceeded $1.6M and were <$100 000 per 1 QALY gained compared with prophylaxis if initial costs were <$1.7M. Results were not sensitive to variation of all other parameters over clinically plausible ranges. In a probabilistic sensitivity analysis simultaneously varying all parameters 3000 times over parameter distributions, gene therapy was dominant in 92% of model iterations. Treatment of severe hemophilia A with gene therapy is likely to be cost-saving or cost-effective compared with FVIII prophylaxis.
© 2018 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures
References
-
- Mannucci PM, Tuddenham EG. The hemophilias--from royal genes to gene therapy. N Engl J Med. 2001;344(23):1773-1779. - PubMed
-
- Soucie JM, Evatt B, Jackson D; The Hemophilia Surveillance System Project Investigators. Occurrence of hemophilia in the United States. Am J Hematol. 1998;59(4):288-294. - PubMed
-
- Skinner MW. Haemophilia: provision of factors and novel therapies: World Federation of Hemophilia goals and achievements. Br J Haematol. 2011;154(6):704-714. - PubMed
-
- Collins PW, Björkman S, Fischer K, et al. . Factor VIII requirement to maintain a target plasma level in the prophylactic treatment of severe hemophilia A: influences of variance in pharmacokinetics and treatment regimens. J Thromb Haemost. 2010;8(2):269-275. - PubMed
-
- Oladapo AO, Epstein JD, Williams E, Ito D, Gringeri A, Valentino LA. Health-related quality of life assessment in haemophilia patients on prophylaxis therapy: a systematic review of results from prospective clinical trials. Haemophilia. 2015;21(5):e344-e358. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
