

Evaluation of the Concurrent Trajectories of Cardiometabolic Risk Factors in the 14 Years Before Dementia
- PMID: 30043038
- PMCID: PMC6233804
- DOI: 10.1001/jamapsychiatry.2018.2004
Evaluation of the Concurrent Trajectories of Cardiometabolic Risk Factors in the 14 Years Before Dementia
Abstract
Importance: Cardiometabolic risk factors have been associated with an increased risk of dementia; yet, the optimal targets and time window for the management of cardiometabolic health to prevent dementia remain unknown.
Objectives: To model concurrently and compare the trajectories of cardiometabolic risk factors up to 14 years preceding diagnosis in individuals with dementia and matched controls free of dementia.
Design, setting, and participants: A case-control study nested within the Three-City study, a French population-based cohort of older persons (≥65 years), included 6 home visits with neuropsychological testing between 1999 and 2014. Data analysis was performed in September 2017. A total of 785 incident dementia cases and 3140 controls matched by sex, age, educational level, and cohort center at the time of diagnosis were evaluated.
Exposures: Repeated measures of body mass index (BMI) and systolic (SBP) and diastolic (DBP) blood pressure, high-density lipoprotein (HDL-C) and low-density lipoprotein cholesterol (LDL-C), triglycerides, and glycemia levels between 1999 and 2014.
Main outcomes and measures: Incidence of dementia based on systematic detection and validated diagnosis.
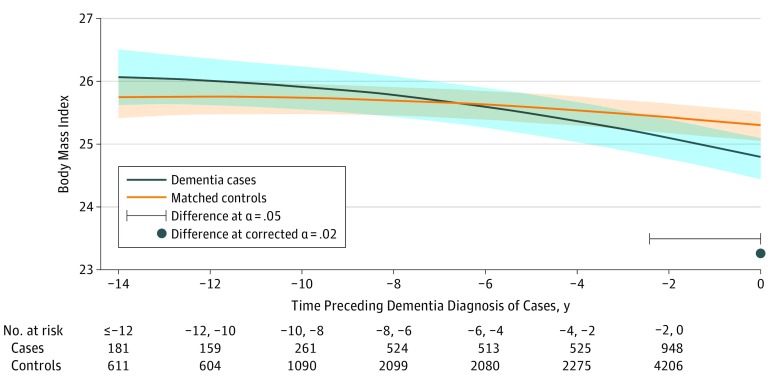
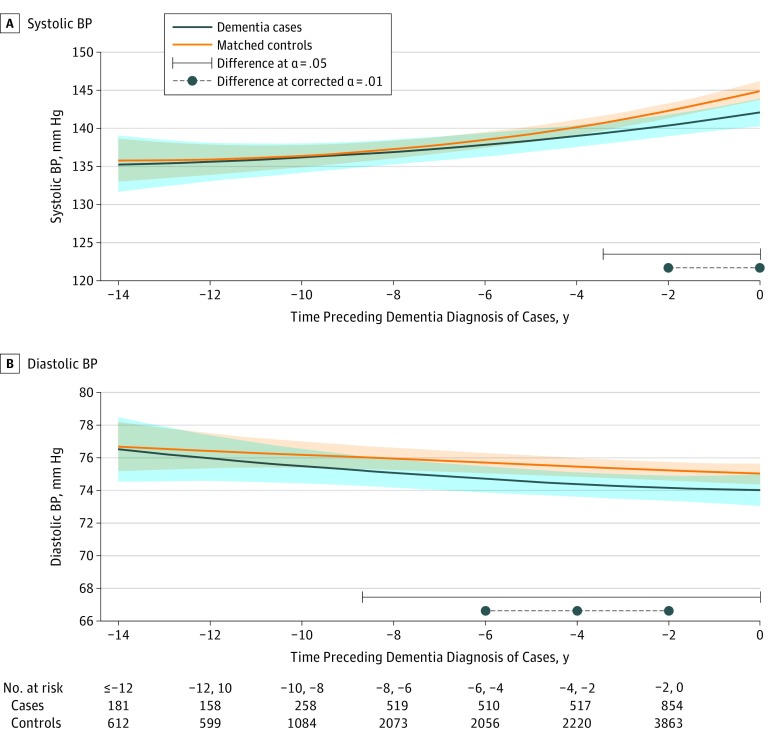
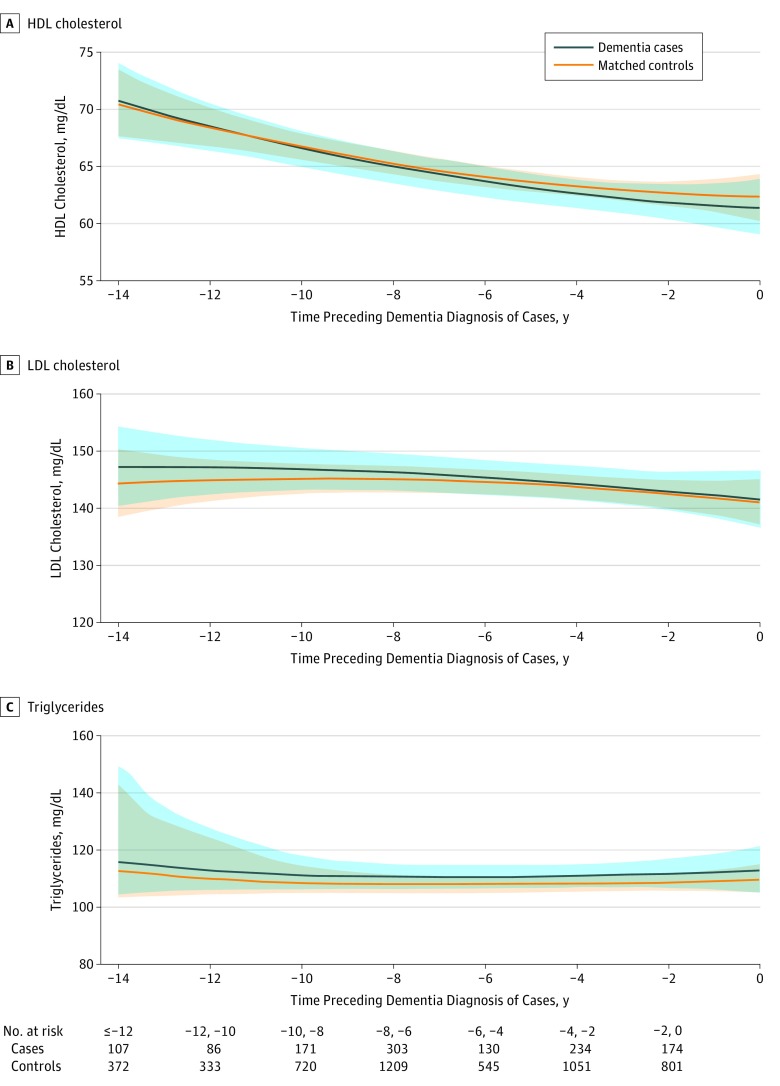
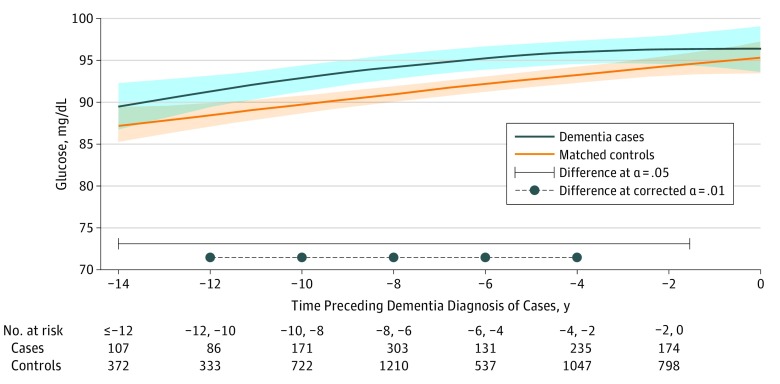
Results: A total of 785 cases and 3140 controls (2530 [65%] women; mean [SD] age, 76 [5] years) were included in the study. Cases presented a faster decline in BMI, slower increase of SBP and constantly lower DBP. Mean values (95% CI) 14 years before diagnosis (-14 years) and at diagnosis (year 0) for the most common profile were BMI, 26.1 (25.6-26.5) and 24.8 (24.5-25.1) for a case, and 25.7 (25.4-26.1) and 25.3 (25.0-25.5) for a control; for SBP, 135.2 (131.8-138.7) and 142.1 (140.3-143.9) mm Hg for a case, and 135.8 (132.9-138.6) and 144.9 (143.7-146.1) mm Hg for a control; for DBP, 76.5 (74.7-78.5) and 74.0 (73.1-74.9) mm Hg for a case, and 76.7 (75.1-78.3) and 75.0 (74.2-75.7) mm Hg for a control. In contrast, glycemia was higher among cases (mean fasting glucose values [95% CI] at -14 years and year 0: 89.4 [86.9-92.1] and 96.4 [93.7-99.3] mg/dL for a case, and 87.1 [85.1-89.2] and 95.3 [93.5-97.1] mg/dL for a control), with a significant case-control difference from -1.6 to -14 years prior to diagnosis. There were no significant case-control differences in trajectories of blood lipid levels (mean values [95% CI] at -14 years and year 0: for HDL-C, 70.6 [67.6-73.9] and 61.3 [58.9-63.8] mg/dL for a case, and 70.4 [67.5-73.3] and 62.3 [60.2-64.3] mg/dL for a control; for LDL-C: 147.2 [140.5-154.5] and 141.6 [136.6-146.7] mg/dL for a case, and 144.3 [138.7-150.4] and 141.2 [137.5-145.2] mg/dL for a control; for triglycerides: 115.5 [103.6-149.1] and 112.6 [104.8-120.9] mg/dL for a case, and 112.5 [103.8-144.4] and 109.7 [105.0-114.8] mg/dL for a control).
Conclusions and relevance: In this large cohort of older persons, BMI declined in prodromal dementia, possibly reflecting early preclinical changes. Lower BP prior to dementia may reflect both a consequence and a contributing factor for the disease, whereas higher blood glucose levels may constitute a risk factor for dementia in the older age range. Overall, these findings suggest that elevated glycemia, low BP, and weight loss may be primary targets for the management of cardiometabolic health for primary and secondary prevention of dementia in the older age range.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
