

Association Between the New York Sepsis Care Mandate and In-Hospital Mortality for Pediatric Sepsis
- PMID: 30043064
- PMCID: PMC6500448
- DOI: 10.1001/jama.2018.9071
Association Between the New York Sepsis Care Mandate and In-Hospital Mortality for Pediatric Sepsis
Abstract
Importance: The death of a pediatric patient with sepsis motivated New York to mandate statewide sepsis treatment in 2013. The mandate included a 1-hour bundle of blood cultures, broad-spectrum antibiotics, and a 20-mL/kg intravenous fluid bolus. Whether completing the bundle elements within 1 hour improves outcomes is unclear.
Objective: To determine the risk-adjusted association between completing the 1-hour pediatric sepsis bundle and individual bundle elements with in-hospital mortality.
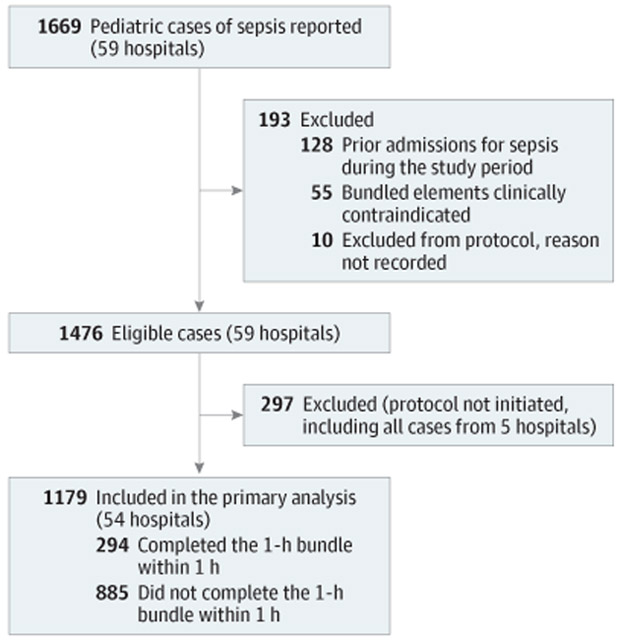
Design, settings, and participants: Statewide cohort study conducted from April 1, 2014, to December 31, 2016, in emergency departments, inpatient units, and intensive care units across New York State. A total of 1179 patients aged 18 years and younger with sepsis and septic shock reported to the New York State Department of Health who had a sepsis protocol initiated were included.
Exposures: Completion of a 1-hour sepsis bundle within 1 hour compared with not completing the 1-hour sepsis bundle within 1 hour.
Main outcomes and measures: Risk-adjusted in-hospital mortality.
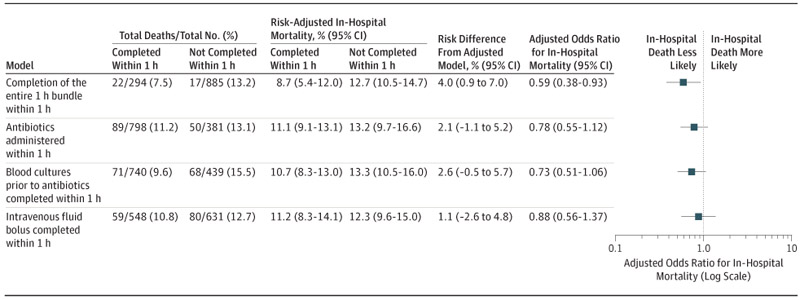
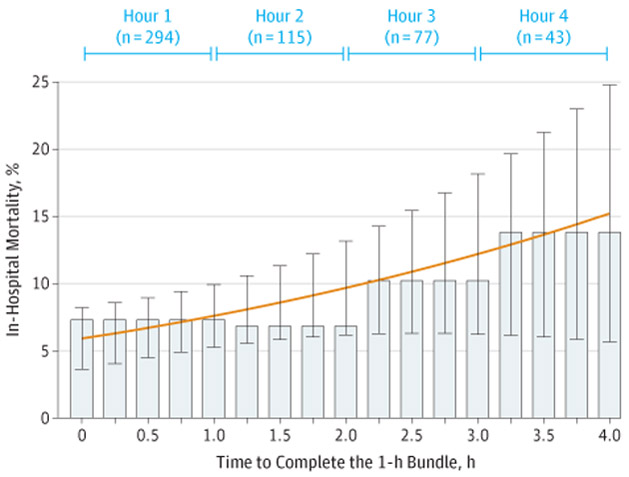
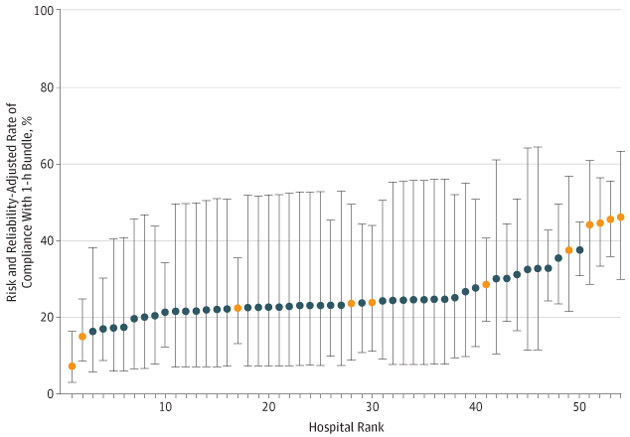
Results: Of 1179 patients with sepsis reported at 54 hospitals (mean [SD] age, 7.2 [6.2] years; male, 54.2%; previously healthy, 44.5%; diagnosed as having shock, 68.8%), 139 (11.8%) died. The entire sepsis bundle was completed in 1 hour in 294 patients (24.9%). Antibiotics were administered to 798 patients (67.7%), blood cultures were obtained in 740 patients (62.8%), and the fluid bolus was completed in 548 patients (46.5%) within 1 hour. Completion of the entire bundle within 1 hour was associated with lower risk-adjusted odds of in-hospital mortality (odds ratio [OR], 0.59 [95% CI, 0.38 to 0.93], P = .02; predicted risk difference [RD], 4.0% [95% CI, 0.9% to 7.0%]). However, completion of each individual bundle element within 1 hour was not significantly associated with lower risk-adjusted mortality (blood culture: OR, 0.73 [95% CI, 0.51 to 1.06], P = .10; RD, 2.6% [95% CI, -0.5% to 5.7%]; antibiotics: OR, 0.78 [95% CI, 0.55 to 1.12], P = .18; RD, 2.1% [95% CI, -1.1% to 5.2%], and fluid bolus: OR, 0.88 [95% CI, 0.56 to 1.37], P = .56; RD, 1.1% [95% CI, -2.6% to 4.8%]).
Conclusions and relevance: In New York State following a mandate for sepsis care, completion of a sepsis bundle within 1 hour compared with not completing the 1-hour sepsis bundle within 1 hour was associated with lower risk-adjusted in-hospital mortality among patients with pediatric sepsis and septic shock.
Conflict of interest statement
Figures
Comment in
-
Bundled Strategies for the Care of Children With Presumed Sepsis.JAMA. 2018 Jul 24;320(4):345-346. doi: 10.1001/jama.2018.9183. JAMA. 2018. PMID: 30043043 No abstract available.
-
Sepsis Bundles and Mortality Among Pediatric Patients.JAMA. 2018 Dec 4;320(21):2271. doi: 10.1001/jama.2018.16748. JAMA. 2018. PMID: 30512094 Free PMC article. No abstract available.
References
-
- Dellinger RP, Levy MM, Rhodes A, et al. Surviving Sepsis Campaign Guidelines Committee including The Pediatric Subgroup. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med. 2013;39(2):165–228. doi: 10.1007/s00134-012-2769-8 - DOI - PMC - PubMed
-
- Dwyer J. An infection, unnoticed, turns unstoppable. The New York Times. https://www.nytimes.com/2012/07/12/nyregion/in-rory-stauntons-fight-for-.... Published July11, 2012. Accessed July20, 2017.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
