

Clinical, Ultrasound, and Predictability Outcomes Following Certolizumab Pegol Treatment (with Methotrexate) in Patients with Moderate-to-Severe Rheumatoid Arthritis: 52-Week Results from the CZP-SPEED Study
- PMID: 30043210
- PMCID: PMC6096970
- DOI: 10.1007/s12325-018-0751-8
Clinical, Ultrasound, and Predictability Outcomes Following Certolizumab Pegol Treatment (with Methotrexate) in Patients with Moderate-to-Severe Rheumatoid Arthritis: 52-Week Results from the CZP-SPEED Study
Abstract
Introduction: To assess the impact of certolizumab pegol (CZP) treatment on clinical, patient-reported, and musculoskeletal ultrasound outcomes and to determine the treatment response time point most predictive of long-term outcomes in Italian patients with rheumatoid arthritis (RA).
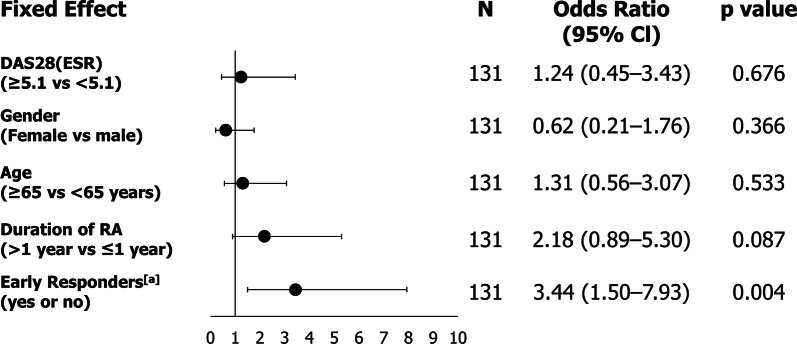
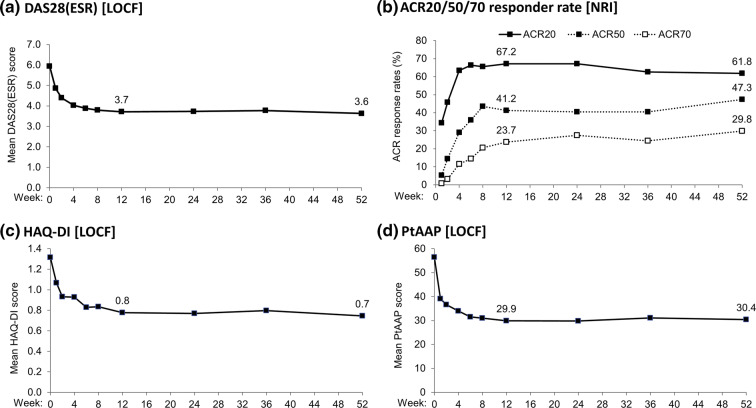
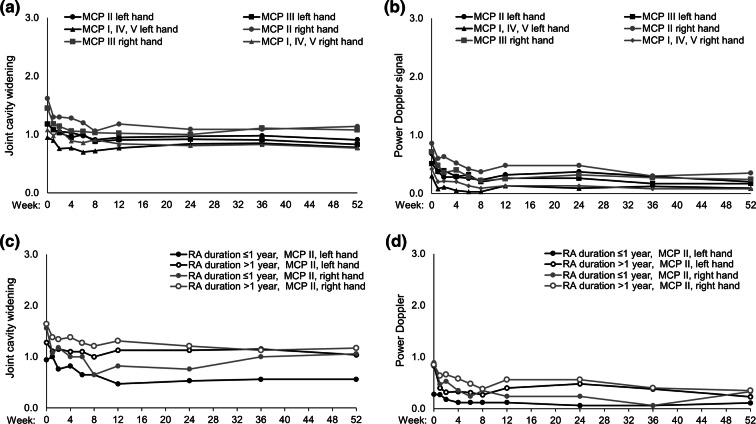
Methods: CZP-SPEED (NCT01443364) was a 52-week, open-label, prospective, interventional, multicenter study. Biologic-naïve patients with moderate-to-severe active RA, who had failed at least one DMARD treatment, received CZP (400 mg at weeks 0, 2, and 4, then 200 mg every 2 weeks) concomitantly with methotrexate. The primary objective was to identify the time point of clinical response {decrease in 28-joint Disease Activity Score [DAS28(ESR)] ≥ 1.2} most predictive of a clinical response at week 52. Additional clinical and patient-reported outcomes were measured. Power Doppler (PD) ultrasound was used to assess synovial effusion, synovial proliferation, PD signal, cartilage damage, and bone erosion according to international guidelines.
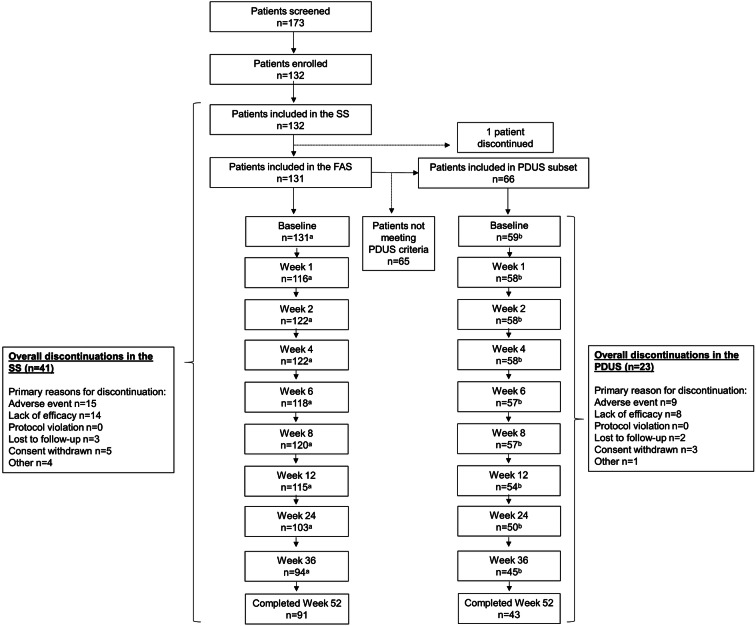
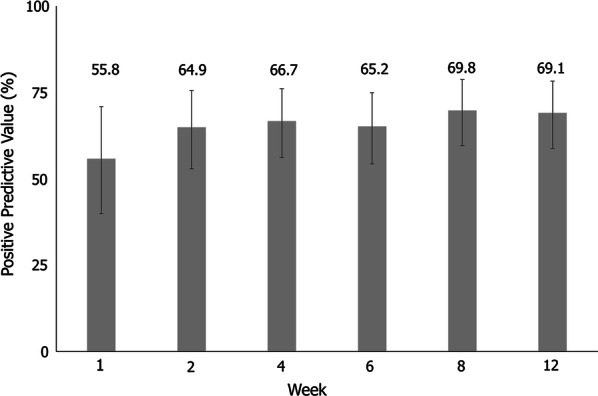
Results: A total of 132 patients were enrolled and received CZP; 91/132 (69%) completed to week 52. Predicted 52-week responses for early responders (week 2 onwards) were between 65% and 70%. Rapid improvements in joint cavity widening and PD signal were observed to week 8 and maintained to week 52. Cartilage damage and bone erosion were stable over 52 weeks. No new safety signals were identified.
Conclusion: In Italian CZP-treated patients with moderate-to-severe RA, week 12 clinical responses may be predictive of long-term response at week 52. Rapid improvements in clinical, patient-reported, and musculoskeletal ultrasound outcomes were maintained to week 52. These data may aid rheumatologists to make earlier treatment decisions.
Trial registration: ClinicalTrials.gov identifier, NCT01443364.
Funding: UCB Pharma.
Keywords: Anti-TNF; Certolizumab pegol; Patient-reported outcome; Predictability; Rheumatoid arthritis; Rheumatology; Ultrasound.
Conflict of interest statement
Piercarlo Sarzi-Puttini: Speaker fees; Emilio Filippucci: Speaker fees: AbbVie, BMS, Celgene, Roche, UCB Pharma; Luca Idolazzi: Speaker fees from Celgene, AbbVie, UCB Pharma, and Janssen; Pablo Talavera: Employee of UCB Pharma; Thomas Kumke: Employee of UCB Pharma; Walter Grassi: Consultancies, speaker fees and/or honoraria: AbbVie, BMS, Gruenthal Menarini, MSD, Novartis, Pfizer, and UCB Pharma. Pier Luigi Meroni, Alberto Batticciotto, Orazio De Lucia and Silvano Adami have nothing to disclose.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
