

Personalized prediction model for seizure-free epilepsy with levetiracetam therapy: a retrospective data analysis using support vector machine
- PMID: 30043454
- PMCID: PMC6177722
- DOI: 10.1111/bcp.13720
Personalized prediction model for seizure-free epilepsy with levetiracetam therapy: a retrospective data analysis using support vector machine
Abstract
Aims: To predict the probability of a seizure-free (SF) state in patients with epilepsy (PWEs) after treatment with levetiracetam and to identify the clinical and electroencephalographic (EEG) factors that affect outcomes.
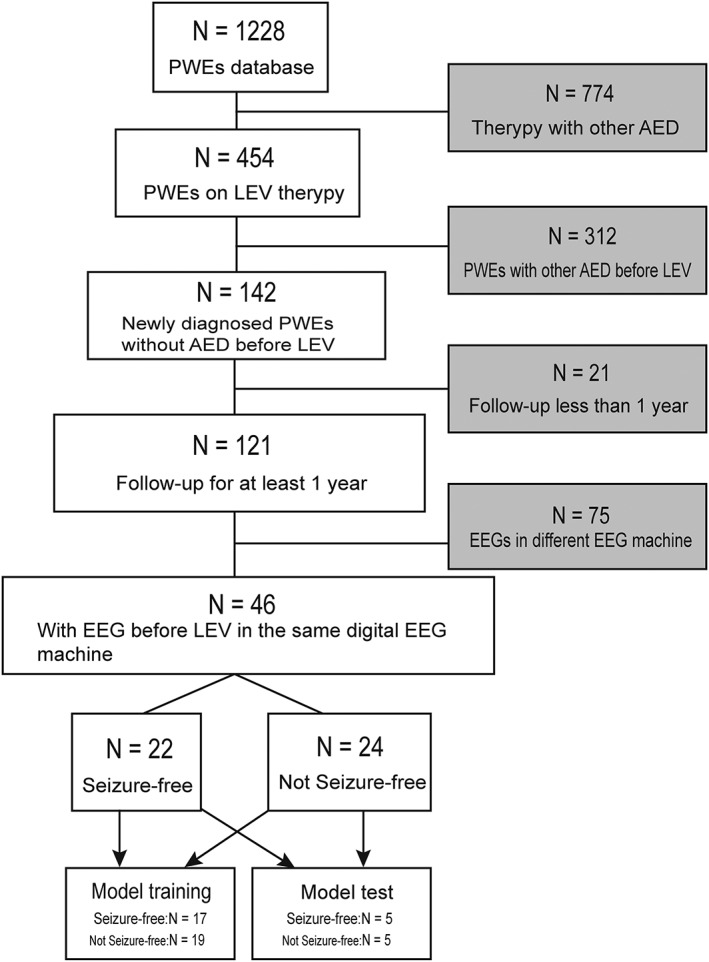
Methods: Retrospective analysis of PWEs treated with levetiracetam for 3 years identified 22 patients who were SF and 24 who were not. Before starting levetiracetam, 11 clinical factors and four EEG features (sample entropy of α, β, θ, δ) were identified. Overall, 80% of each the two groups were chosen to establish a support vector machine (SVM) model with 5-fold cross-validation, hold-out validation and jack-knife validation. The other 20% were used to predict the efficacy of levetiracetam. The mean impact value (MIV) algorithm was used to rank the relativity between factors and outcomes.
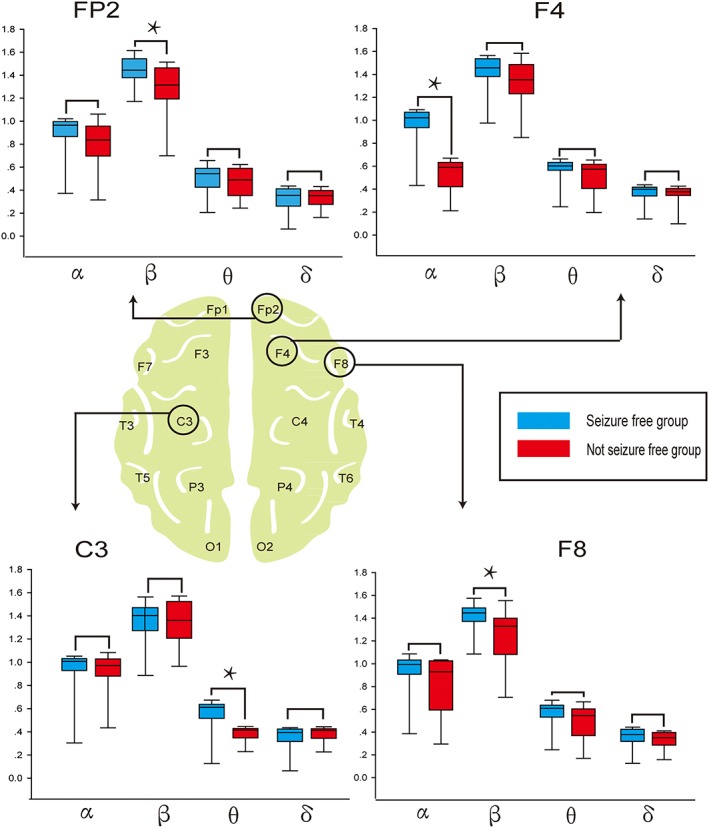
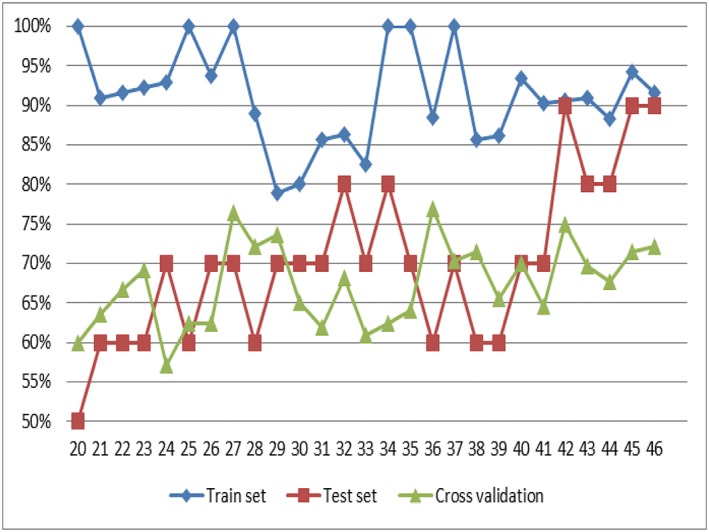
Results: Compared with SF patients, not SF patients displayed a specific decrease in EEG sample entropy in α band from the F4 channel, β band from Fp2 and F8 channels, θ band from C3 channel (P < 0.05). The SVM model based on the clinical and EEG features yielded 72.2% accuracy of 5-fold cross-validation, 75.0% accuracy of jack-knife validation, 67.7% accuracy of hold-out validation in the training set and had a high prediction accuracy of 90% in test set (sensitivity was 100%, area under the receiver operating characteristic curve was 0.96). The feature of β band from Fp2 weighs heavily in the prediction model according to the mean impact value algorithm.
Conclusions: The efficacy of levetiracetam on newly diagnosed PWEs could be predicted using an SVM model, which could guide antiepileptic drug selection.
Keywords: effectiveness; epilepsy; methodology; neuroscience; therapeutics.
© 2018 The British Pharmacological Society.
Figures

References
-
- Glauser T, Ben‐Menachem E, Bourgeois B, Cnaan A, Guerreiro C, Kalviainen R, et al Updated ILAE evidence review of antiepileptic drug efficacy and effectiveness as initial monotherapy for epileptic seizures and syndromes. Epilepsia 2013; 54: 551–563. - PubMed
-
- Dlugos DJ, Sammel MD, Strom BL, Farrar JT. Response to first drug trial predicts outcome in childhood temporal lobe epilepsy. Neurology 2001; 57: 2259–2264. - PubMed
-
- Perucca E, Tomson T. The pharmacological treatment of epilepsy in adults. The Lancet Neurology 2011; 10: 446–456. - PubMed
-
- Ben‐Menachem E. Medical management of refractory epilepsy – practical treatment with novel antiepileptic drugs. Epilepsia 2014; 55 (Suppl. 1): 3–8. - PubMed
-
- Kwan P, Brodie MJ. Clinical trials of antiepileptic medications in newly diagnosed patients with epilepsy. Neurology 2003; 60 (11 Suppl. 4): S2–S12. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
