

Fetal megacystis: a lot more than LUTO
- PMID: 30043466
- PMCID: PMC6593717
- DOI: 10.1002/uog.19182
Fetal megacystis: a lot more than LUTO
Abstract
Objective: Fetal megacystis presents a challenge in terms of counseling and management because of its varied etiology and evolution. The aim of this study was to present a comprehensive overview of the underlying etiologies and structural anomalies associated with fetal megacystis.
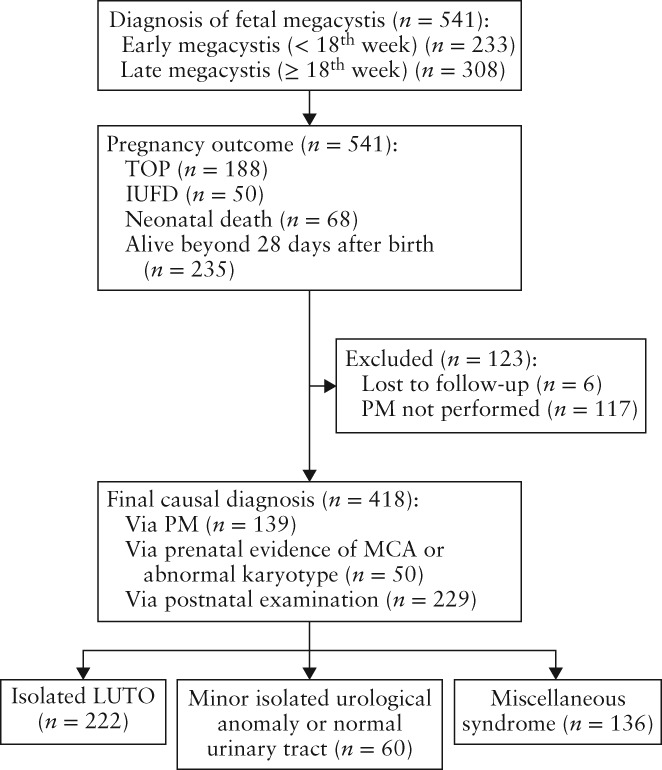
Methods: This was a retrospective multicenter study of cases referred to the fetal medicine unit of one of the eight academic hospitals in The Netherlands with a diagnosis of fetal megacystis. For each case, data on and measurements of fetal urinary tract and associated structural anomalies were collected. All available postmortem examinations and postnatal investigations were reviewed in order to establish the final diagnosis. In the first trimester, fetal megacystis was defined as longitudinal bladder diameter (LBD) ≥ 7 mm, and in the second and third trimesters as an enlarged bladder failing to empty during an extended ultrasound examination lasting at least 40 min.
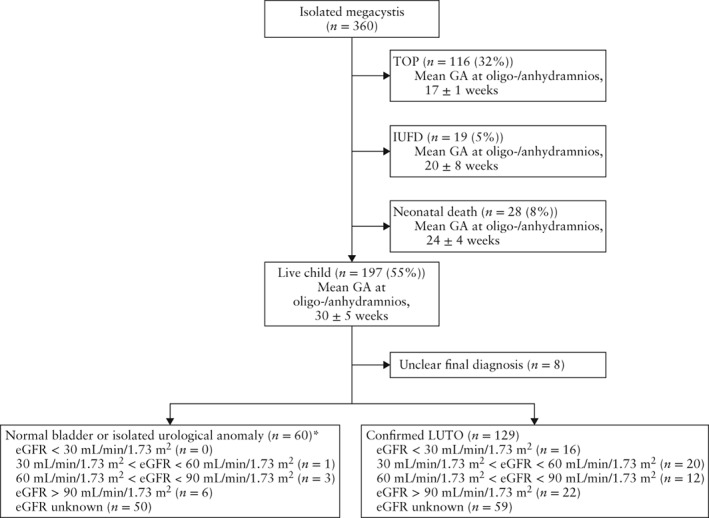
Results: Of the 541 pregnancies with fetal megacystis, it was isolated (or solely accompanied by other signs of lower urinary tract obstruction (LUTO)) in 360 (67%) cases and associated with other abnormal ultrasound findings in 181 (33%) cases. The most common associated ultrasound anomaly was an increased nuchal translucency thickness (22%), followed by single umbilical artery (10%) and cardiac defect (10%). A final diagnosis was established in 418 cases, including 222 (53%) cases with isolated LUTO and 60 (14%) infants with normal micturition or minor isolated urological anomalies. In the remaining 136 (33%) cases, concomitant developmental or chromosomal abnormality or genetic syndrome was diagnosed. Overall, 40 chromosomal abnormalities were diagnosed, including trisomy 18 (n = 24), trisomy 21 (n = 5), Turner syndrome (n = 5), trisomy 13 (n = 3) and 22q11 deletion (n = 3). Thirty-two cases presented with anorectal malformations involving the anus, rectum and urogenital tract. In cases with confirmed urethral and anal atresia, megacystis occurred early in pregnancy and the bladder appeared severely distended (the LBD (in mm) was equal to or greater than twice the gestational age (in weeks)). Fetal macrosomia was detected in six cases and an overgrowth syndrome was detected in four cases, comprising two infants with Beckwith-Wiedemann syndrome and two with Sotos syndrome. Megacystis-microcolon-intestinal hypoperistalsis syndrome was diagnosed in five (1%) cases and prenatally suspected only in one case.
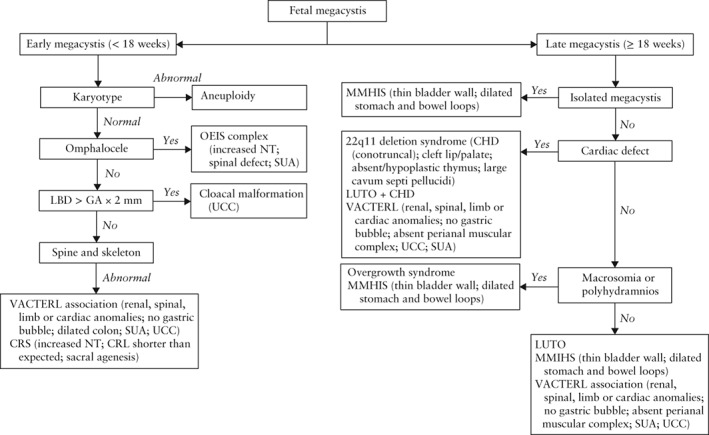
Conclusions: Although the main cause of fetal megacystis is LUTO, an enlarged fetal bladder can also be present as a concomitant finding of miscellaneous genetic syndromes, developmental disturbances and chromosomal abnormalities. We provide an overview of the structural anomalies and congenital disorders associated with fetal megacystis and propose a practical guide for the differential diagnosis of genetic syndromes and chromosomal and developmental abnormalities in pregnancies presenting with fetal megacystis, focusing on the morphological examination of the fetus. © 2018 The Authors. Ultrasound in Obstetrics & Gynecology published by John Wiley & Sons Ltd on behalf of the International Society of Ultrasound in Obstetrics and Gynecology.
Keywords: anorectal malformation; fetal megacystis; lower urinary tract obstruction.
© 2018 The Authors. Ultrasound in Obstetrics & Gynecology published by John Wiley & Sons Ltd on behalf of the International Society of Ultrasound in Obstetrics and Gynecology.
Figures
References
-
- McHugo J, Whittle M. Enlarged fetal bladders: aetiology, management and outcome. Prenat Diagn 2001; 21: 958–963. - PubMed
-
- Sebire NJ, Von Kaisenberg C, Rubio C, Snijders RJM, Nicolaides KH. Fetal megacystis at 10–14 weeks of gestation. Ultrasound Obstet Gynecol 1996; 8: 387–390. - PubMed
-
- Taghavi K, Sharpe C, Stringer MD. Fetal megacystis: A systematic review. J Pediatr Urol 2017; 13: 7–15. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
