

Challenges in Orphan Drug Development: Identification of Effective Therapy for Thyroid-Associated Ophthalmopathy
- PMID: 30044728
- PMCID: PMC8415464
- DOI: 10.1146/annurev-pharmtox-010617-052509
Challenges in Orphan Drug Development: Identification of Effective Therapy for Thyroid-Associated Ophthalmopathy
Abstract
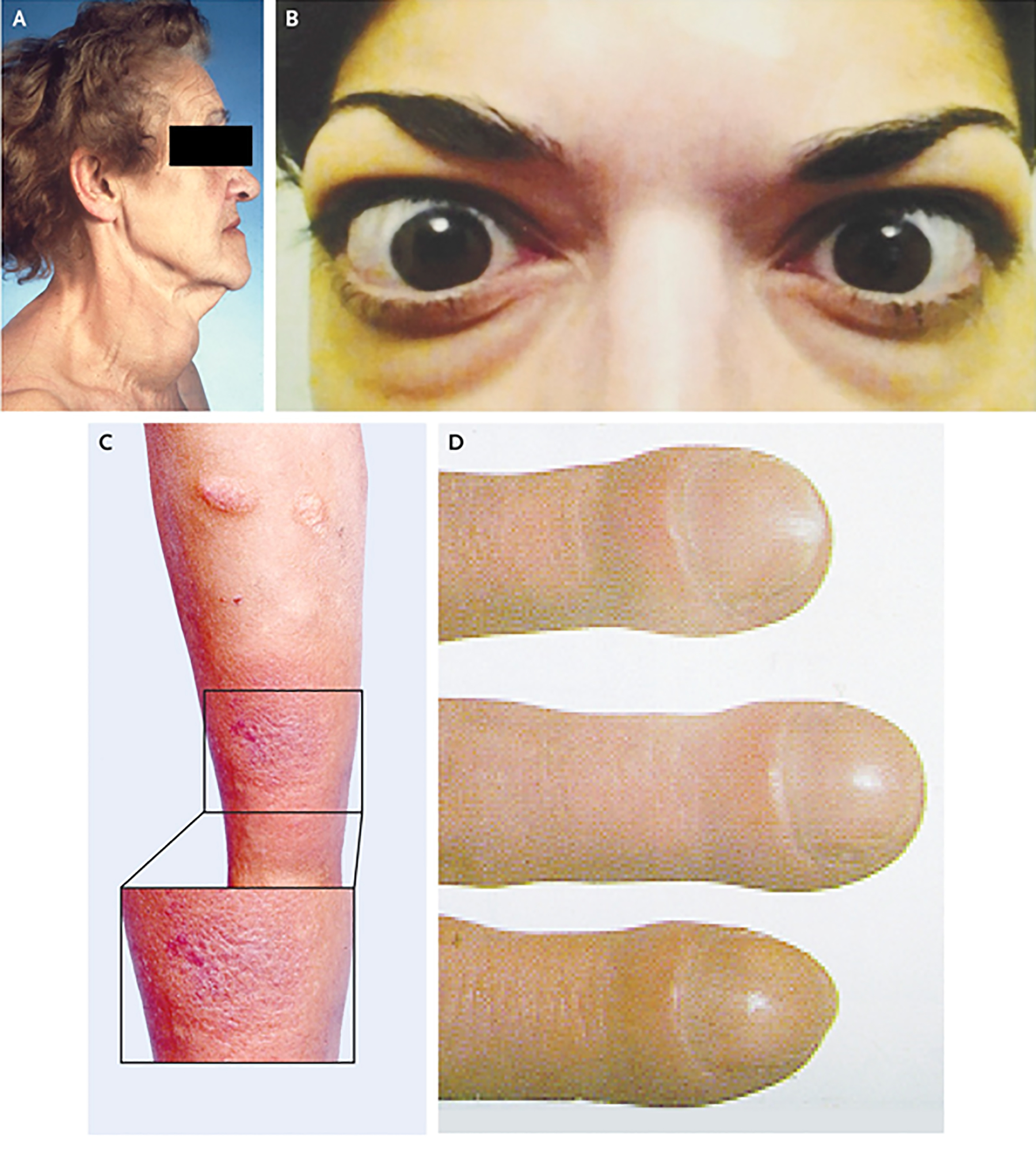
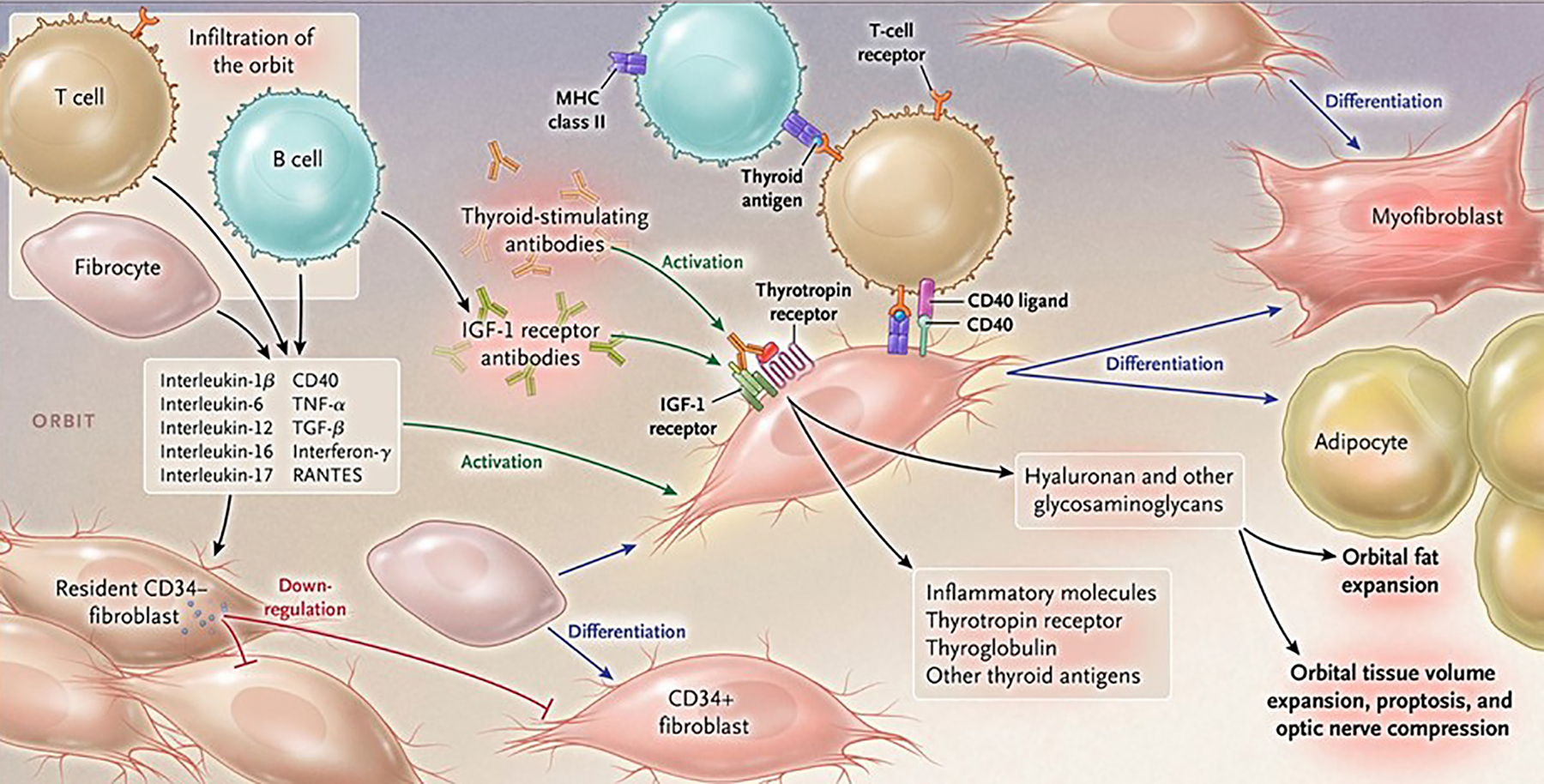
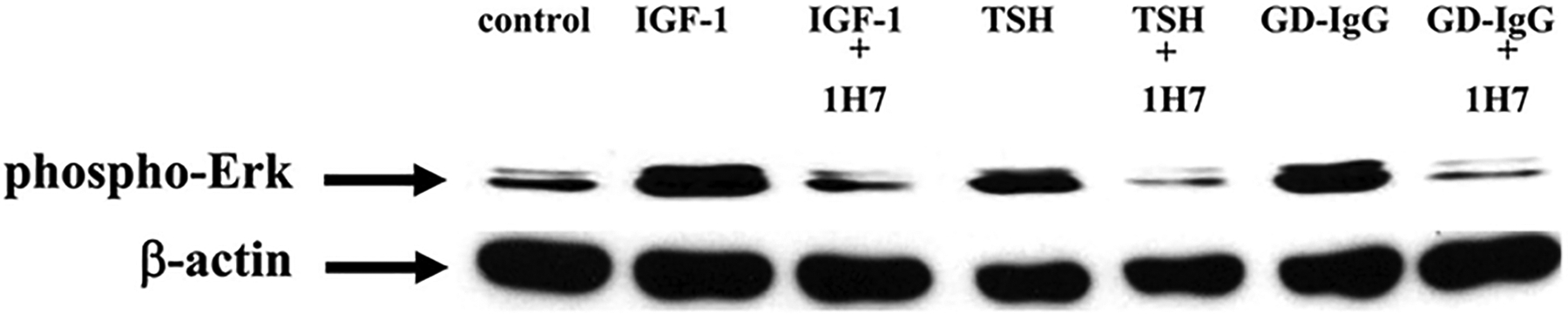
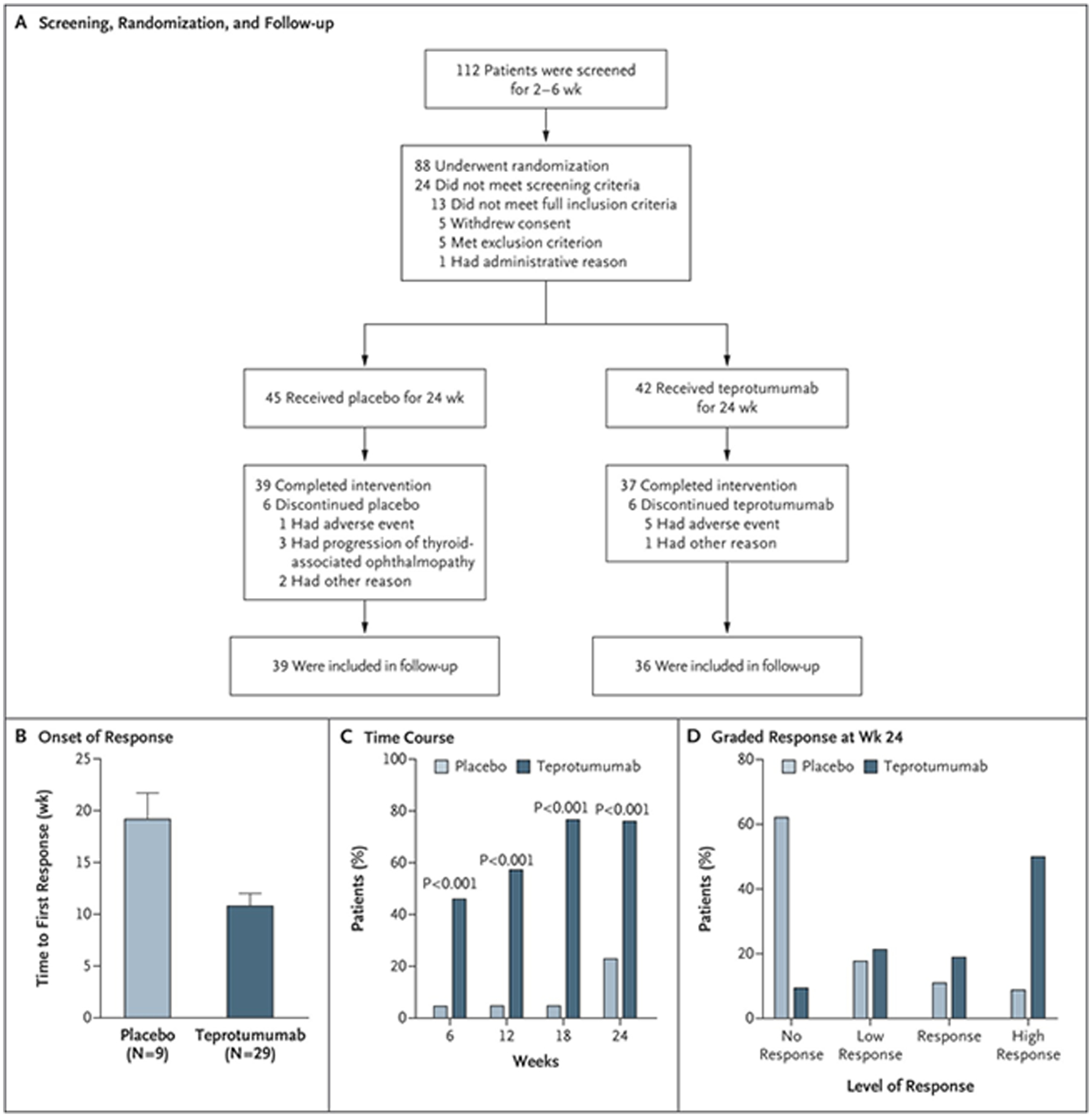
Thyroid-associated ophthalmopathy (TAO), the ocular manifestation of Graves' disease, is a process in which orbital connective tissues and extraocular muscles undergo inflammation and remodeling. The condition seems to result from autoimmune responses to antigens shared by the thyroid and orbit. The thyrotropin receptor (TSHR), expressed at low levels in orbital tissues, is a leading candidate antigen. Recent evidence suggests that another protein, the insulin-like growth factor-I receptor (IGF-IR), is overexpressed in TAO, and antibodies against IGF-IR have been detected in patients with the disease. Furthermore, TSHR and IGF-IR form a physical and functional complex, and signaling initiated at TSHR requires IGF-IR activity. Identification of therapy for this rare disease has proven challenging and currently relies on nonspecific and inadequate agents, thus representing an important unmet need. A recently completed therapeutic trial suggests that inhibiting IGF-IR activity with a monoclonal antibody may be an effective and safe treatment for active TAO.
Keywords: Graves’ disease; autoimmune; monoclonal antibody; signaling.
Conflict of interest statement
Conflicts
The author has been issued patents related to the detection of antibody-mediated inflammatory auto-immune disorders (US 6936426), the diagnosis and therapy of antibody-mediated inflammatory autoimmune disorders (US 7998681 and US 8153121), and diagnostic methods related to Graves’ disease and other autoimmune disorders (US 8178304). He was previously a paid consultant for River Vision.
Figures

References
-
- Smith TJ, Hegedus L. 2016. Graves’ Disease. N. Engl. J. Med 375:1552–65 - PubMed
-
- Rundle FF, Wilson CW. 1945. Development and course of exophthalmos and ophthalmoplegia in Graves’ disease with special reference to the effect of thyroidectomy. Clin. Sci 5:177–94 - PubMed
-
- Bartalena L, Piantanida E. 2016. Cigarette smoking: number one enemy for Graves ophthalmopathy. Pol. Arch. Med. Wewn 126:725–6 - PubMed
-
- Chu X, Pan CM, Zhao SX, Liang J, Gao GQ, et al.2011. A genome-wide association study identifies two new risk loci for Graves’ disease. Nat. Genet 43:897–901 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
