

Characteristics, outcome and treatments with cranial pachymeningitis: A multicenter French retrospective study of 60 patients
- PMID: 30045263
- PMCID: PMC6078725
- DOI: 10.1097/MD.0000000000011413
Characteristics, outcome and treatments with cranial pachymeningitis: A multicenter French retrospective study of 60 patients
Erratum in
-
Characteristics, outcome and treatments with cranial pachymeningitis: A multicenter French retrospective study of 60 patients: Erratum.Medicine (Baltimore). 2018 Aug;97(33):e12063. doi: 10.1097/MD.0000000000012063. Medicine (Baltimore). 2018. PMID: 30113504 Free PMC article. No abstract available.
Abstract
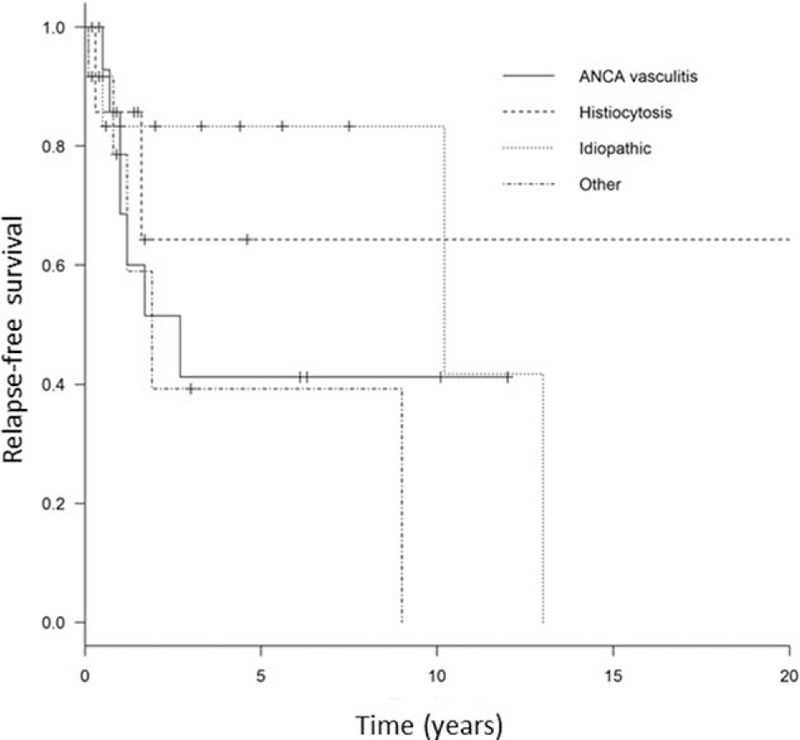
The aim of this study was to determine the characteristics, treatment, and outcome according to each etiology of pachymeningitis.We conducted a retrospective multicenter French nationwide study between 2000 and 2016 to describe the characteristics, outcome, and treatment of pachymeningitis.We included 60 patients (median age 55.5 years; interquartile range [IQR] 30-80, female/male ratio 0.43). Neurologic signs were present in 59 patients (98%) and consisted of headache in 43 (72%), cranial nerve palsy in 33 (55%), confusion in 10 (17%), seizures in 7 (12%), and focal neurologic signs in 9 (15%). Fever and weight loss were present in 8 (13%) and 13 cases (22%), respectively. Cerebral venous thrombosis was present in 8 cases (13%). Analysis of cerebrospinal fluid showed moderate hyperproteinorachia (median 0.68 g/L; IQR 0.46-3.2) with or without pleiocytosis. Diagnosis included idiopathic pachymeningitis (n = 18; 30%); granulomatosis with polyangiitis (n = 13; 17%); Erdheim-Chester disease (n = 10; 17%); IgG4-related disease and tuberculosis (n = 3; 5% each); Rosai-Dofman disease, microscopic polyangiitis, and sarcoidosis (n = 2, 3% each); cryptococcal meningitis, Lyme disease, ear-nose-throat infection, postlumbar puncture, low spinal-fluid pressure syndrome, and lymphoma (n = 1 each). We found no difference in demographics and neurologic presentation among idiopathic pachymeningitis, Erdheim-Chester disease, and granulomatosis with polyangiitis. In contrast, frequencies were lower with idiopathic pachymeningitis than Erdheim-Chester disease for general signs (6% and 40%, respectively, P = .041) and complete neurologic response (0% vs 39%, P = .045).The detection of extraneurologic signs and routine screening are needed to classify the pachymeningitis origin. Prospective studies are warranted to determine the best treatment in each case.
Figures
References
-
- Fain O, Seror O, Wirth JF, et al. Cranial pachymeningitis [in French]. Rev Med Interne 1999;20:234–46. - PubMed
-
- Lu LX, Della-Torre E, Stone JH, et al. IgG4-related hypertrophic pachymeningitis: clinical features, diagnostic criteria, and treatment. JAMA Neurol 2014;71:785–93. - PubMed
-
- Yokoseki A, Saji E, Arakawa M, et al. Hypertrophic pachymeningitis: significance of myeloperoxidase anti-neutrophil cytoplasmic antibody. Brain 2014;137:520–36. - PubMed
-
- Yonekawa T, Murai H, Utsuki S, et al. A nationwide survey of hypertrophic pachymeningitis in Japan. J Neurol Neurosurg Psychiatry 2014;85:732–9. - PubMed
-
- Fujimoto M, Kira J, Murai H, et al. Hypertrophic cranial pachymeningitis associated with mixed connective tissue disease; a comparison with idiopathic and infectious pachymeningitis. Intern Med 1993;32:510–2. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
