

Lymphovascular invasion can be better than pathologic complete response to predict prognosis in breast cancer treated with neoadjuvant chemotherapy
- PMID: 30045313
- PMCID: PMC6078671
- DOI: 10.1097/MD.0000000000011647
Lymphovascular invasion can be better than pathologic complete response to predict prognosis in breast cancer treated with neoadjuvant chemotherapy
Abstract
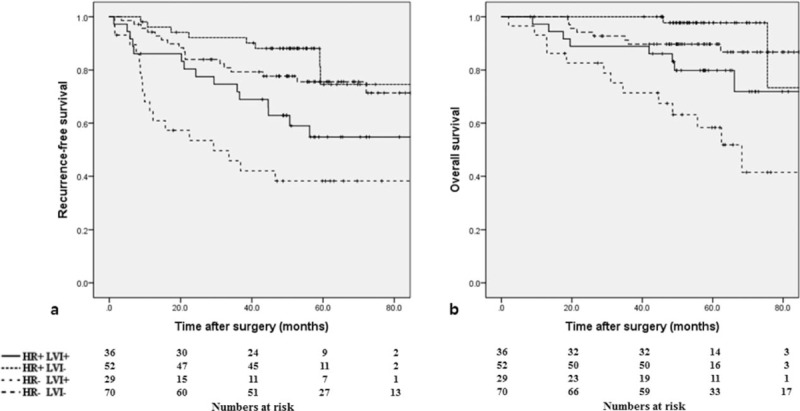
Lymphovascular invasion (LVI) has been a predictor of worse survival outcomes in breast cancer. However, the role of LVI compared than pathologic complete response (pCR) following neoadjuvant chemotherapy (NAC) remains unclear. The aim of this study was to examine the association between LVI and survival outcomes and clinicopathological features in patients with breast cancer treated with NAC. We retrospectively analyzed 187 patients with breast cancer treated with NAC and surgery between 2005 and 2013 in our institution. Kaplan-Meier analyses were used to assess recurrence-free survival (RFS) and overall survival (OS). Median follow-up was 57.9 months. Mastectomy (vs breast conserving surgery [BCS]; hazard ratio [HR], 1.791; 95% confidence interval [CI], 1.022-3.139; P = .042), ypN1-3 stage (vs ypN0 stage; HR, 2.561; 95% CI, 1.247-5.261; P = .010), and LVI (vs no LVI; HR, 2.041; 95% CI, 1.170-3.562; P = .012) were associated with worse RFS. Mastectomy (vs BCS; HR, 2.768; 95% CI, 1.173-6.535; P = .020), LVI (vs no LVI; HR, 3.474; 95% CI, 1.646-7.332, P = .001), and human epidermal growth factor receptor 2 overexpression type (vs luminal A type; HR, 11.360; 95% CI, 1.501-85.972; P = .019) were associated with worse OS. Patients with LVI and hormone receptor-negative cancer had the worst RFS (P < .001) and OS (P < .001). LVI more than pCR in surgical breast cancer specimens obtained after NAC was a significant independent prognostic factor. Patients with hormonal receptor-negative cancer and LVI had unfavorable survival outcomes. We suggest that patients with hormone receptor-negative cancer and LVI should receive short-term follow-up and appropriate management.
Figures
References
-
- Sachelarie I, Grossbard ML, Chadha M, et al. Primary systemic therapy of breast cancer. Oncologist 2006;11:574–89. - PubMed
-
- Tsuji W, Teramukai S, Ueno M, et al. Prognostic factors for survival after first recurrence in breast cancer: a retrospective analysis of 252 recurrent cases at a single institution. Breast Cancer 2014;21:86–95. - PubMed
-
- Love RR, Duc NB, Dinh NV, et al. Young age as an adverse prognostic factor in premenopausal women with operable breast cancer. Clin Breast Cancer 2002;2:294–8. - PubMed
-
- Schwartz AM, Henson DE, Chen D, et al. Histologic grade remains a prognostic factor for breast cancer regardless of the number of positive lymph nodes and tumor size: a study of 161 708 cases of breast cancer from the SEER Program. Arch Pathol Lab Med 2014;138:1048–52. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
