

Post-traumatic right carotid-cavernous fistula resulting in symptoms in the contralateral eye: a case report and literature review
- PMID: 30045703
- PMCID: PMC6060543
- DOI: 10.1186/s12886-018-0863-6
Post-traumatic right carotid-cavernous fistula resulting in symptoms in the contralateral eye: a case report and literature review
Abstract
Background: To report a case of a carotid-cavernous fistula (CCF) that occurred after a motor vehicle accident and review the uniqueness of this case and the main confusing points for the diagnosis of such cases.
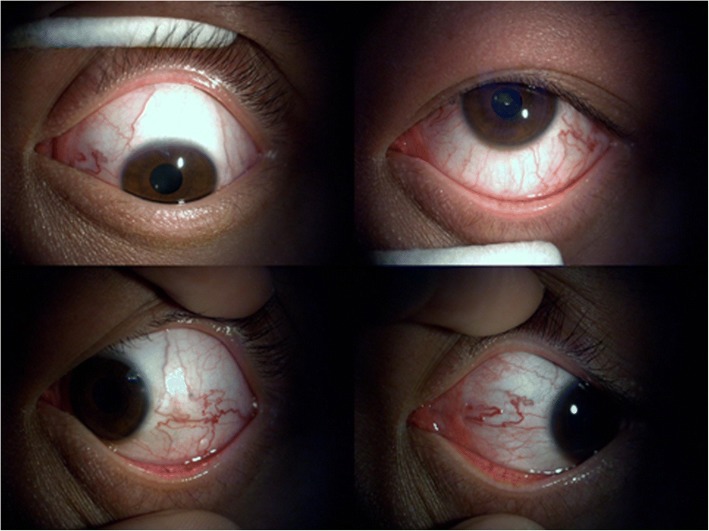
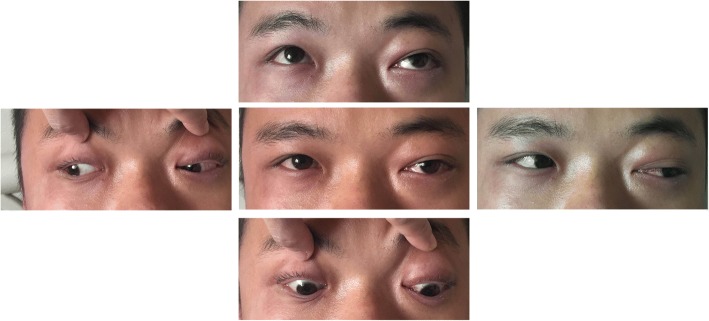
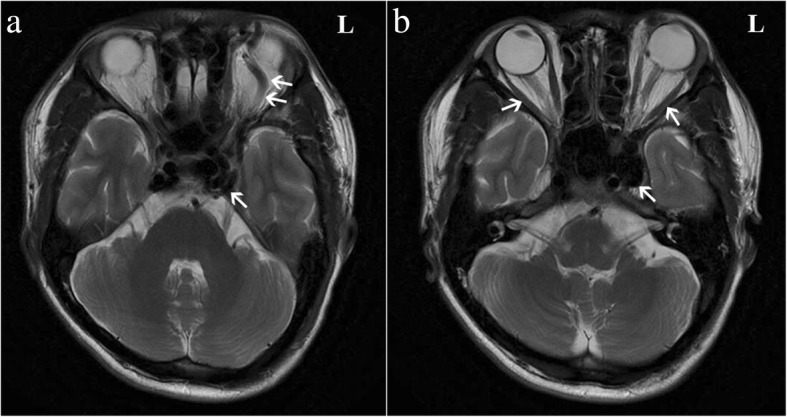
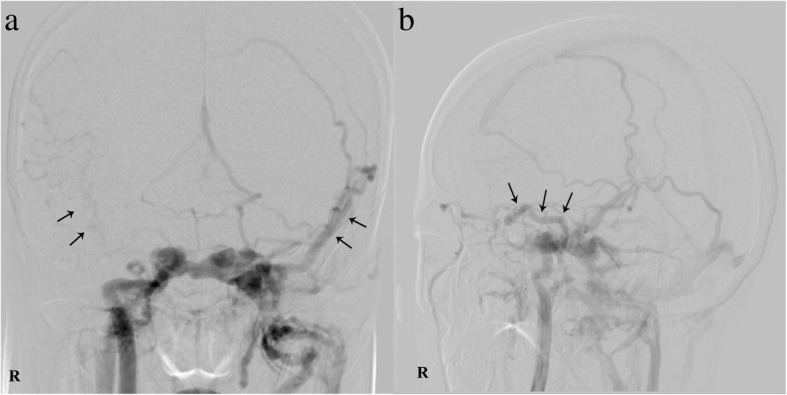
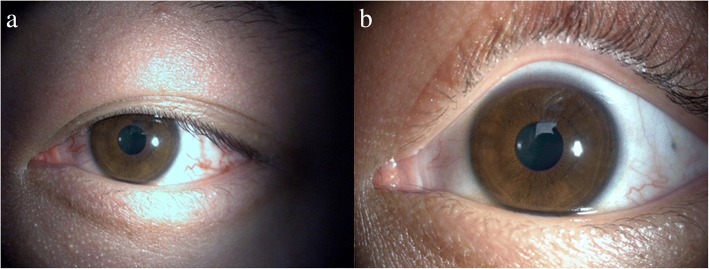
Case presentation: A 22-year-old man complained of left eyelid swelling, eye redness, visual decrease and occasional headache after motor vehicle accident 4 months prior during which he experienced a head injury. He was initially thought to have glaucoma, but he was finally diagnosed with a right CCF based on magnetic resonance imaging (MRI) and digital subtraction angiography (DSA). Timely embolization surgery resulted in obvious relief of the ocular symptoms and an improved prognosis.
Conclusion: This is the first reported case of a post-traumatic unilateral CCF with contralateral symptoms in direct CCF, it is very infrequent and deserves our attention. We should maintain high suspicion of CCF and confirm the diagnosis by DSA when managing such patients to prevent serious consequences. Early diagnosis and treatment can improve the prognosis of patients.
Keywords: CCF; Contralateral; DSA; Trauma.
Conflict of interest statement
Ethics approval and consent to participate
This study followed the tenets of the Declaration of Helsinki and approved by the Ethics Committee of the First Affiliated Hospital of Jinan University. Written informed consent was obtained from the participant.
Consent for publication
Written informed consent was obtained from the patient for publication of this case and any accompanying images. A copy of written consent is available for review by the Executive Editor of this journal.
Competing interest
The authors declare that they have no competing interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Liang W, Xiaofeng Y, Weiguo L, Wusi Q, Gang S, Xuesheng Z. Traumatic carotid cavernous fistula accompanying basilar skull fracture: a study on the incidence of traumatic carotid cavernous fistula in the patients with basilar skull fracture and the prognostic analysis about traumatic carotid cavernous fistula. J Trauma. 2007;63(5):1014–1020. doi: 10.1097/TA.0b013e318154c9fb. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
