

Clinical outcomes during anticoagulant therapy in fragile patients with venous thromboembolism
- PMID: 30046687
- PMCID: PMC6058265
- DOI: 10.1002/rth2.12036
Clinical outcomes during anticoagulant therapy in fragile patients with venous thromboembolism
Abstract
Background: Subgroup analyses from randomized trials suggested favorable results for the direct oral anticoagulants in fragile patients with venous thromboembolism (VTE). The frequency and natural history of fragile patients with VTE have not been studied yet.
Objectives: To compare the clinical characteristics, treatment and outcomes during the first 3 months of anticoagulation in fragile vs non-fragile patients with VTE.
Methods: Retrospective study using consecutive patients enrolled in the RIETE (Registro Informatizado Enfermedad TromboEmbolica) registry. Fragile patients were defined as those having age ≥75 years, creatinine clearance (CrCl) levels ≤50 mL/min, and/or body weight ≤50 kg.
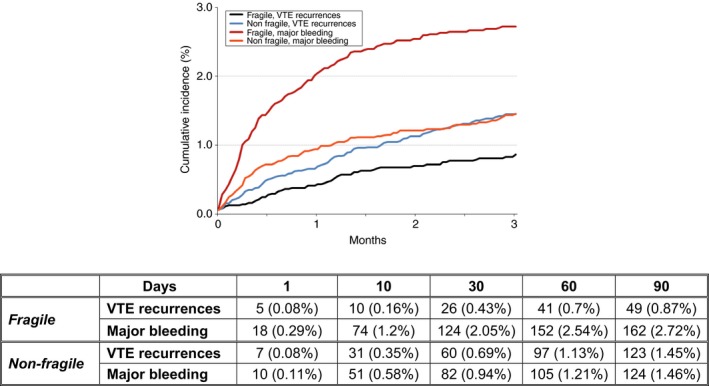
Results: From January 2013 to October 2016, 15 079 patients were recruited. Of these, 6260 (42%) were fragile: 37% were aged ≥75 years, 20% had CrCl levels ≤50 mL/min, and 3.6% weighed ≤50 kg. During the first 3 months of anticoagulant therapy, fragile patients had a lower risk of VTE recurrences (0.78% vs 1.4%; adjusted odds ratio [OR]: 0.52; 95% confidence intervals [CI]: 0.37-0.74) and a higher risk of major bleeding (2.6% vs 1.4%; adjusted OR: 1.41; 95% CI: 1.10-1.80), gastrointestinal bleeding (0.86% vs 0.35%; adjusted OR: 1.84; 95% CI: 1.16-2.92), haematoma (0.51% vs 0.07%; adjusted OR: 5.05; 95% CI: 2.05-12.4), all-cause death (9.2% vs 3.5%; adjusted OR: 2.02; 95% CI: 1.75-2.33), or fatal PE (0.85% vs 0.35%; adjusted OR: 1.77; 95% CI: 1.10-2.85) than the non-fragile.
Conclusions: In real life, 42% of VTE patients were fragile. During anticoagulation, they had fewer VTE recurrences and more major bleeding events than the non-fragile.
Keywords: anticoagulants; hemorrhage; mortality; recurrences; venous thromboembolism.
Figures
References
-
- Schulman S, Kearon C, Kakkar AK, et al.; RE‐COVER Study Group . Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N Engl J Med. 2009;361:2342–52. - PubMed
-
- Agnelli G, Buller HR, Cohen A, et al.; AMPLIFY Investigators . Oral apixaban for the treatment of acute venous thromboembolism. N Engl J Med. 2013;369:799–808. - PubMed
-
- Bauersachs R, Berkowitz SD, Brenner B, et al.; EINSTEIN Investigators . Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med. 2010;363:2499–510. - PubMed
-
- Büller HR, Prins MH, Lensin AWA, et al.; EINSTEIN‐PE Investigators . Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med. 2012;366:1287–97. - PubMed
-
- Büller HR, Décousus H, Grosso MA, et al.; Hokusai‐VTE Investigators . Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism. N Engl J Med. 2013;369:1406–15. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
