

Acute infection as a trigger for incident venous thromboembolism: Results from a population-based case-crossover study
- PMID: 30046710
- PMCID: PMC6055491
- DOI: 10.1002/rth2.12065
Acute infection as a trigger for incident venous thromboembolism: Results from a population-based case-crossover study
Abstract
Background: A bidirectional relation exists between acute infection and immobilization, and both are triggers for venous thromboembolism (VTE). To what extent the association between infection and VTE-risk is explained by immobilization is unknown.
Aims: To investigate the impact of hospitalization with acute infection on the VTE-risk in patients with and without concomitant immobilization, and to explore the differential impact of respiratory- (RTI) and urinary- (UTI) tract infections on the risk of deep vein thrombosis (DVT) and pulmonary embolism (PE).
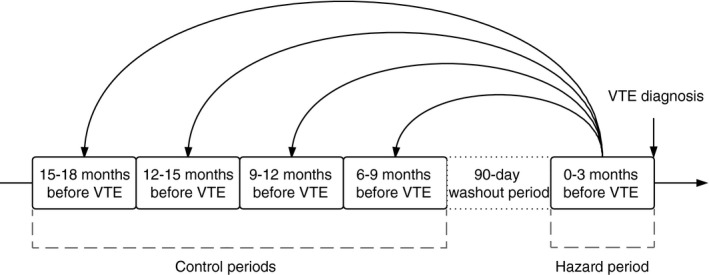
Methods: We conducted a case-crossover study of VTE-patients (n = 707) recruited from a general population. Hospitalizations and VTE-triggers were registered during the 90 days before a VTE (hazard period) and in four preceding 90-day control periods. Conditional logistic regression was used to estimate odds ratios (ORs) for VTE according to triggers.
Results: Acute infection was registered in 267 (37.8%) of the hazard periods and in 107 (3.8%) of the control periods, corresponding to a high VTE-risk after infection (OR 24.2, 95% CI 17.2-34.0), that was attenuated to 15-fold increased after adjustment for immobilization. The risk was 20-fold increased after infection without concomitant immobilization, 73-fold increased after immobilization without infection, and 141-fold increased with the two combined. The risk of PE was apparently higher after RTIs (OR 48.3, 95% CI 19.4-120.0) than UTIs (OR 12.6, 95% CI 6.4-24.7), but diminished in sensitivity analyses excluding uncertain RTI diagnoses.
Conclusions: Our findings suggest that hospitalization with infection is a strong VTE-trigger also in non-immobilized patients. Infection and immobilization had a synergistic effect on the VTE-risk.
Keywords: deep vein thrombosis; immobilization; infection; pulmonary embolism; venous thromboembolism.
Figures
References
-
- Heit JA, Melton LJ 3rd, Lohse CM, et al. Incidence of venous thromboembolism in hospitalized patients vs community residents. Mayo Clin Proc. 2001;76:1102–10. - PubMed
-
- Heit JA, O'Fallon WM, Petterson TM, et al. Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: a population‐based study. Arch Intern Med. 2002;162:1245–8. - PubMed
-
- Feland N, Wendelboe AM, McCumber MD, et al. Hospital associated venous thromboembolism in Oklahoma County. Blood. 2016;128:416.
LinkOut - more resources
Full Text Sources
Other Literature Sources
