

Extended anticoagulation for unprovoked venous thromboembolism
- PMID: 30046758
- PMCID: PMC6046599
- DOI: 10.1002/rth2.12121
Extended anticoagulation for unprovoked venous thromboembolism
Abstract
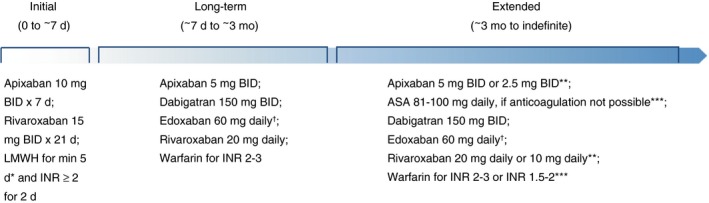
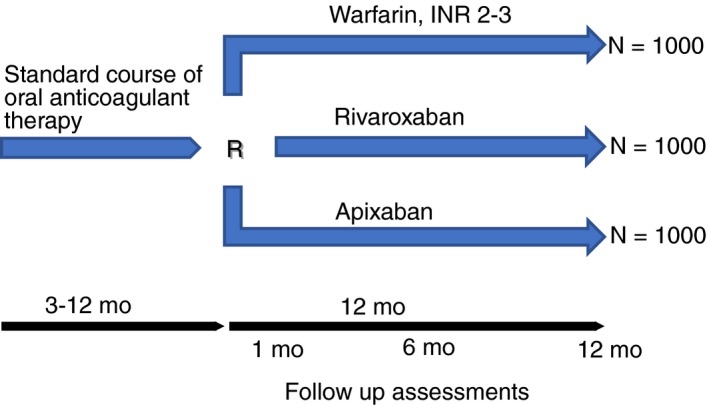
After completing anticoagulation therapy for acute venous thromboembolism (VTE), patients with unprovoked VTE are at increased risk of recurrent thrombotic events. Recent studies suggest a risk of nearly 10% in the first year after stopping anticoagulants and 30% at 8 years. Therefore, it is important to consider extended anticoagulation for secondary prevention in these high-risk patients. While several oral anticoagulants are available for this purpose, there is limited information available regarding the optimal agent to minimize bleeding risks and maximize efficacy at VTE prevention. This review article summarizes the evidence available for Vitamin-K antagonists (VKAs) and direct oral anticoagulants (DOACs) for extended treatment of VTE. We also introduce the COVET trial, the first head-to-head comparison of VKAs to DOACs, rivaroxaban and apixaban, for extended management of unprovoked VTE.
Keywords: anticoagulation; bleeding; recurrent; secondary prevention; venous thromboembolism; venous thrombosis.
Figures
References
-
- White RH. The epidemiology of venous thromboembolism. Circulation. 2003;107:I‐4–8. - PubMed
-
- Heit J. The epidemiology of venous thromboembolism in the community: implications for prevention and management. J Thromb Thrombolysis. 2006;21:23–9. - PubMed
-
- Kyrle PA, Minar E, Bialonczyk C, Hirschl M, Weltermann A, Eichinger S. The risk of recurrent venous thromboembolism in men and women. N Engl J Med. 2004;350:2558–63. - PubMed
-
- Kearon C, Akl EA, Ornelas J, et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest. 2016;149:315–52. - PubMed
-
- Baglin T, Luddington R, Brown K, Baglin C. Incidence of recurrent venous thromboembolism in relation to clinical and thrombophilic risk factors: prospective cohort study. Lancet. 2003;362:523–6. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
