

Geographic Disparities in Reported US Amyloidosis Mortality From 1979 to 2015: Potential Underdetection of Cardiac Amyloidosis
- PMID: 30046835
- PMCID: PMC6233639
- DOI: 10.1001/jamacardio.2018.2093
Geographic Disparities in Reported US Amyloidosis Mortality From 1979 to 2015: Potential Underdetection of Cardiac Amyloidosis
Abstract
Importance: Cardiac amyloidosis is an underdiagnosed disease and is highly fatal when untreated. Early diagnosis and treatment with the emerging novel therapies significantly improve survival. A comprehensive analysis of amyloidosis-related mortality is critical to appreciate the nature and distribution of underdiagnosis and improve disease detection.
Objective: To evaluate the temporal and regional trends in age-adjusted amyloidosis-related mortality among men and women of various races/ethnicities in the United States.
Design, setting, and participants: In this observational cohort study, death certificate information from the Centers for Disease Control and Prevention's Wide-ranging ONline Data for Epidemiologic Research database and the National Vital Statistics System from 1979 to 2015 was analyzed. A total of 30 764 individuals in the United States with amyloidosis listed as the underlying cause of death and 26 591 individuals with amyloidosis listed as a contributing cause of death were analyzed.
Exposures: Region of residence.
Main outcomes and measures: Age-adjusted mortality rate from amyloidosis per 1 000 000 population stratified by year, sex, race/ethnicity, and state and county of residence.
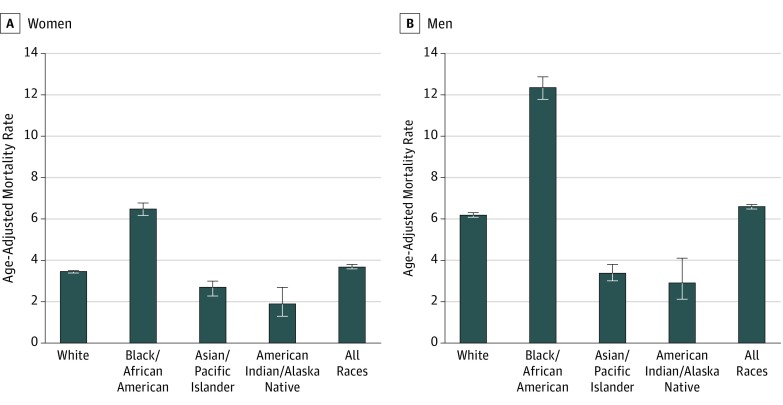
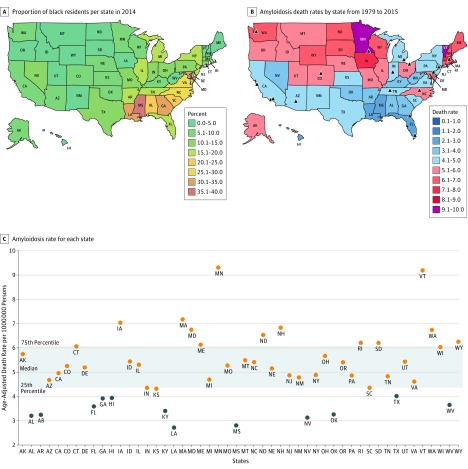
Results: Of the 30 764 individuals with amyloidosis listed as the underlying cause of death, 17 421 (56.6%) were men and 27 312 (88.8%) were 55 years or older. From 1979 to 2015, the reported overall mean age-adjusted mortality rate from amyloidosis as the underlying cause of death doubled from 1.77 to 3.96 per 1 000 000 population (2.32 to 5.43 in men and 1.35 to 2.80 in women). Black men had the highest mortality rate (12.36 per 1 000 000), followed by black women (6.48 per 1 000 000). Amyloidosis contributed to age-adjusted mortality rates as high as 31.73 per 1 000 000 in certain counties. Most southern states reported the lowest US mortality rates despite having the highest proportions of black individuals.
Conclusions and relevance: The increased reported mortality over time and in proximity to amyloidosis centers more likely reflects an overall increase in disease diagnosis rather than increased lethality. The reported amyloidosis mortality is highly variable in different US regions. The lack of higher reported mortality rates in states with a greater proportion of black residents suggests underdiagnosis of amyloidosis, including cardiac forms of the disease, in many areas of the United States. Better understanding of the determinants of geographic and racial disparity in the reporting of amyloidosis deaths are warranted.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
