

The Clinical Significance of Breast-only and Node-only Pathologic Complete Response (pCR) After Neoadjuvant Chemotherapy (NACT): A Review of 20,000 Breast Cancer Patients in the National Cancer Data Base (NCDB)
- PMID: 30048319
- PMCID: PMC6496955
- DOI: 10.1097/SLA.0000000000002953
The Clinical Significance of Breast-only and Node-only Pathologic Complete Response (pCR) After Neoadjuvant Chemotherapy (NACT): A Review of 20,000 Breast Cancer Patients in the National Cancer Data Base (NCDB)
Abstract
Objective: To determine whether the association between overall survival (OS) and response to neoadjuvant chemotherapy (NACT) in breast cancer patients varies with tumor subtype and anatomic extent of pathologic complete response (pCR).
Background: pCR after NACT predicts improved OS in breast cancer, but it is unclear whether pCR limited to the breast or axilla is also associated with OS.
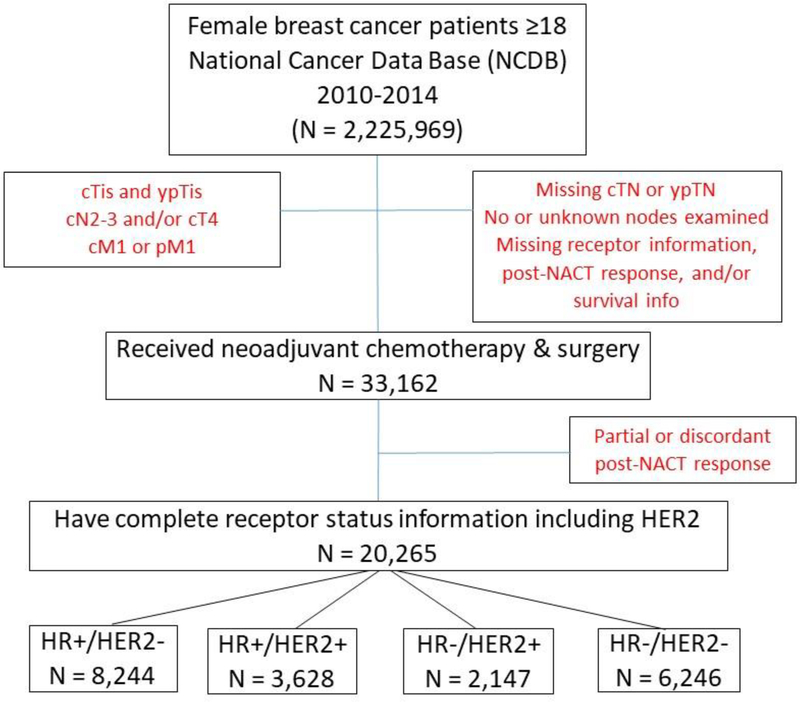
Methods: Women with cT1-3/cN0-1 breast cancer diagnosed in 2010 to 2014 who underwent surgery following NACT were identified in the NCDB and divided into 4 subtypes based on reported hormone receptor (HR) and human epidermal growth factor receptor 2 (HER2) status. Kaplan-Meier curves and Cox proportional hazards models were used to estimate OS. Multivariate logistic regression was used to identify factors associated with post-NACT response, defined as upstage (yp stage>clinical stage); no change (clinical stage = yp stage); overall (breast+axilla, ypT0N0), breast-only (ypT0N1/N1mic), or node-only (ypT1-3N0) pCR.
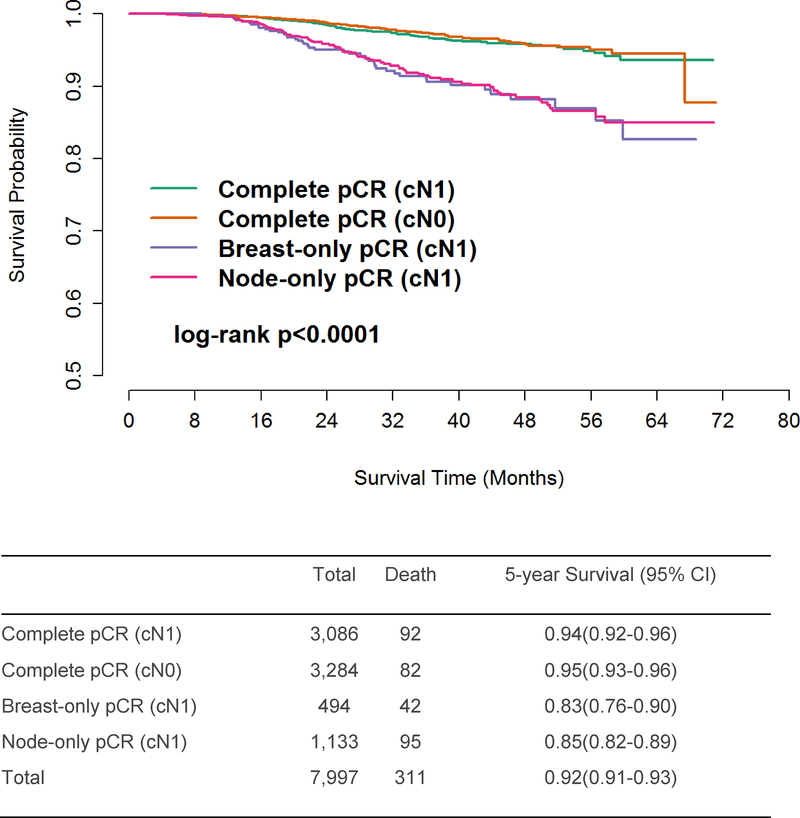
Results: Of 33,162 identified patients, 20,265 experienced overall pCR (n = 6370, 19.2%), breast-only pCR (n = 494, 1.5%), node-only pCR (n = 1133, 3.4%), no stage change (n = 9641, 29.1%), or upstage (n = 2627, 7.9%). Compared with no stage change, breast-only pCR was associated with improved OS in triple-negative disease [hazard ratio = 0.58, 95% confidence interval (95% CI) = 0.37-0.89], and node-only pCR was associated with improved OS in both triple-negative (hazard ratio = 0.55,95% CI = 0.39-0.76) and HR+/HER2- disease (hazard ratio = 0.54, 95% CI = 0.33-0.89). For patients achieving overall (breast+axilla) pCR, unadjusted 5-year OS was 0.94 (95% CI = 0.93-0.95), with no difference between patients who were cN0 (hazard ratio = 0.95, 95% CI = 0.93-0.96) or cN1 (hazard ratio = 0.94, 95% CI = 0.92-0.96) at diagnosis.
Conclusions: In node-positive patients, pCR limited to either the breast or axilla predicts survival for select receptor subtypes. In patients achieving pCR in both the breast and axilla, survival is driven by response to NACT rather than presenting cN stage.
Conflict of interest statement
Figures
References
-
- American Joint Commission on Cancer (AJCC) Staging Manual 2010; 7th:https://cancerstaging.org/references-tools/deskreferences/Pages/default..... Accessed 1 March 2018.
-
- Giuliano AE, Connolly JL, Edge SB, et al. Breast Cancer-Major changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA: a cancer journal for clinicians. 2017;67(4):290–303. - PubMed
-
- Gianni L, Eiermann W, Semiglazov V, et al. Neoadjuvant chemotherapy with trastuzumab followed by adjuvant trastuzumab versus neoadjuvant chemotherapy alone, in patients with HER2-positive locally advanced breast cancer (the NOAH trial): a randomised controlled superiority trial with a parallel HER2-negative cohort. Lancet. 2010;375(9712):377–384. - PubMed
-
- Gianni L, Pienkowski T, Im Y-H, et al. 5-year analysis of neoadjuvant pertuzumab and trastuzumab in patients with locally advanced, inflammatory, or early-stage HER2-positive breast cancer (NeoSphere): a multicentre, open-label, phase 2 randomised trial. Lancet Oncol. 2016;17(6):791–800. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
