

Epidemiology and Costs of Sepsis in the United States-An Analysis Based on Timing of Diagnosis and Severity Level
- PMID: 30048332
- PMCID: PMC6250243
- DOI: 10.1097/CCM.0000000000003342
Epidemiology and Costs of Sepsis in the United States-An Analysis Based on Timing of Diagnosis and Severity Level
Abstract
Objectives: To characterize the current burden, outcomes, and costs of managing sepsis patients in U.S. hospitals.
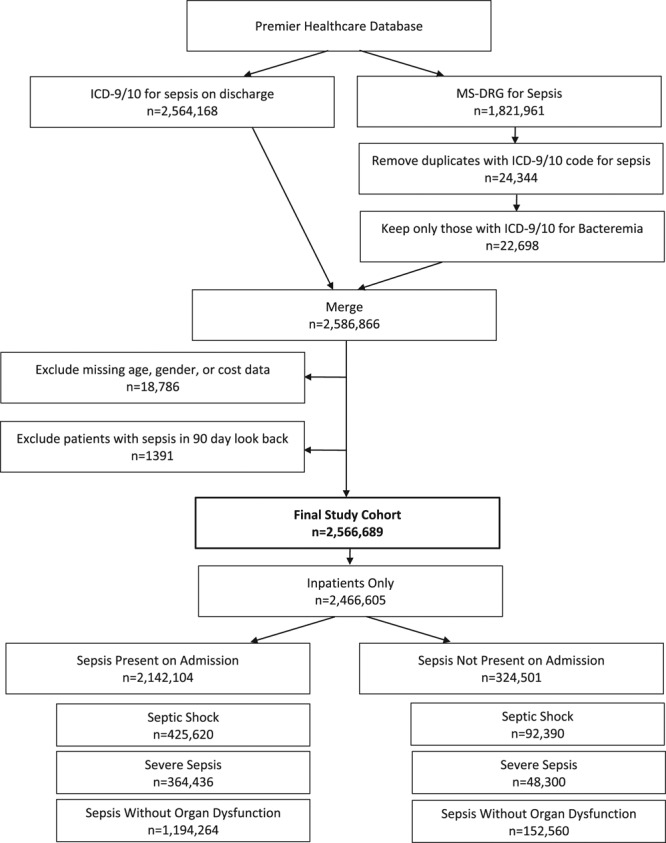
Design: A retrospective observational study was conducted using the Premier Healthcare Database, which represents ~20% of U.S. inpatient discharges among private and academic hospitals. Hospital costs were obtained from billing records per the cost accounting method used by each hospital. Descriptive statistics were performed on patient demographics, characteristics, and clinical and economic outcomes for the index hospitalization and 30-day readmissions.
Setting: Sepsis patient hospitalizations, including inpatient, general ward, and ICU (intermediate and/or step-down).
Patients: Adults over 18 years old with a hospital discharge diagnosis code of sepsis from January 1, 2010, to September 30, 2016.
Interventions: None. This was a retrospective observational study of deidentified data.
Measurements and main results: The final study cohort consisted of 2,566,689 sepsis cases, representing patients with a mean age of 65 years (50.8% female). Overall mortality was 12.5% but varied greatly by severity (5.6%, 14.9%, and 34.2%) for sepsis without organ dysfunction, severe sepsis, and septic shock, respectively. Costs followed a similar pattern increasing by severity level: $16,324, $24,638, and $38,298 and varied widely by sepsis present at admission ($18,023) and not present at admission ($51,022).
Conclusions: The highest burden of incidence and total costs occurred in the lowest severity sepsis cohort population. Sepsis cases not diagnosed until after admission, and those with increasing severity had a higher economic burden and mortality on a case-by-case basis. Methods to improve early identification of sepsis may provide opportunities for reducing the severity and economic burden of sepsis in the United States.
Figures
Comment in
-
Severity and Timing of Onset Drive Economic Costs and Clinical Outcomes With Sepsis.Crit Care Med. 2018 Dec;46(12):2043-2044. doi: 10.1097/CCM.0000000000003376. Crit Care Med. 2018. PMID: 30444807 Free PMC article. No abstract available.
-
Reporting Epidemiologic Studies in Sepsis Combining the International Classification of Diseases, 9th Edition and International Classification of Diseases, 10th Edition Codes.Crit Care Med. 2019 Sep;47(9):e785. doi: 10.1097/CCM.0000000000003794. Crit Care Med. 2019. PMID: 31415318 No abstract available.
-
The authors reply.Crit Care Med. 2019 Sep;47(9):e785-e786. doi: 10.1097/CCM.0000000000003877. Crit Care Med. 2019. PMID: 31415319 No abstract available.
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Crit Care Med 2001; 29:1303–1310. - PubMed
-
- Martin GS, Mannino DM, Eaton S, et al. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med 2003; 348:1546–1554. - PubMed
-
- Liu V, Escobar GJ, Greene JD, et al. Hospital deaths in patients with sepsis from 2 independent cohorts. JAMA 2014; 312:90–92. - PubMed
-
- Hall MJ, Williams SN, DeFrances CJ, et al. Inpatient Care for Septicemia or Sepsis: A Challenge for Patients And Hospitals, 2000–2008. National Center for Health Statistics. Data Brief No. 62. June 2011. Available at: http://www.cdc.gov/nchs/data/databriefs/db62.pdf. Accessed June 24, 2016. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
