

Early predictors of acute hepatitis B progression to liver failure
- PMID: 30048531
- PMCID: PMC6062084
- DOI: 10.1371/journal.pone.0201049
Early predictors of acute hepatitis B progression to liver failure
Abstract
Background and aims: 1~4% of acute hepatitis B (AHB) cases in adults progresses to acute liver failure (ALF).The predictors of ALF and prognosis for patients with ALF are not clear. This study investigated some of predictive and prognostic factors for AHB progression to ALF.
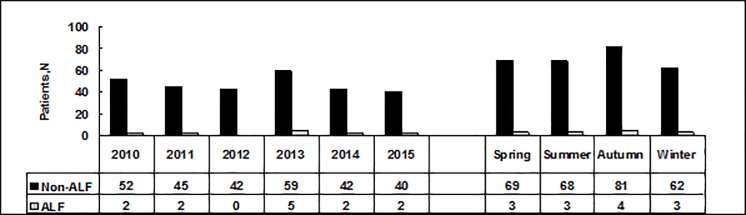
Methods: A retrospective analysis was used to assess the clinical and laboratory features of 293 patients diagnosed with AHB; the patients were divided into the following two groups: ALF (n = 13) and non-ALF (n = 280).
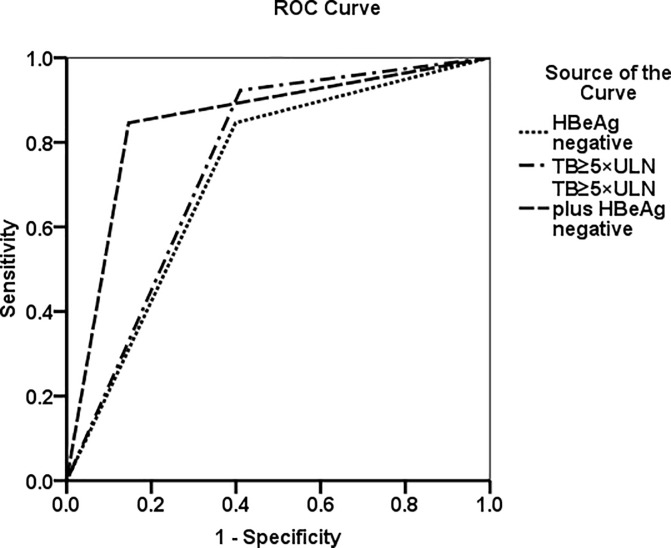
Results: In total,13 of the 293 (4.43%) patients developed ALF (10 recovered、3 died). The variables of age, anti-HBc IgM titers≥10 S/CO, HBeAg negativity, and total bilirubin (TB) at admission were significantly higher in ALF patients than in non-ALF patients. Compared to non-ALF patients, ALF patients had significantly lower values for prothrombin time activity (PTA), serum albumin, and HBV DNA. At discharge, ALF patients had lower TB normalization rates and much faster clearance of HBsAg, HBeAg and HBVDNA than non-ALF patients. In multivariate analysis, TB≥5×upper limit of normal (ULN) and HBeAg negative status were independent predictors for ALF development at admission, with 84.6% sensitivity, 85.7% specificity, a likelihood ratio of 5.91 and an area under the receiver operating characteristics curve (AUROC) of 0.850.Those who died had lower levels of peak PTA (<20%) and higher levels of peak hepatic encephalopathy (HE) grade (III-IV) than those who recovered.
Conclusions: Of the patients with ALF, 23.1% died. TB≥5×ULN and HBeAg negative status were the most effective and practicable factors distinguishing ALF from AHB at admission before the onset of encephalopathy. Peak PTA<20% and/or HE grade III-IV were independent predictors of a high probability of death or a need for transplantation.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Ichai P, Samuel D: Etiology and prognosis of fulminant hepatitis in adults. Liver Transpl. 2008; 14 Suppl 2:S67–79. - PubMed
-
- Dhiman RK, Seth AK, Jain S, Chawla YK, Dilawari JB. Prognostic evaluation of early indicators in fulminant hepatic failure by multivariate analysis. Dig Dis Sci. 1998; 43(6):1311–6. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
