

Hybrid 3D/2D Convolutional Neural Network for Hemorrhage Evaluation on Head CT
- PMID: 30049723
- PMCID: PMC6128745
- DOI: 10.3174/ajnr.A5742
Hybrid 3D/2D Convolutional Neural Network for Hemorrhage Evaluation on Head CT
Abstract
Background and purpose: Convolutional neural networks are a powerful technology for image recognition. This study evaluates a convolutional neural network optimized for the detection and quantification of intraparenchymal, epidural/subdural, and subarachnoid hemorrhages on noncontrast CT.
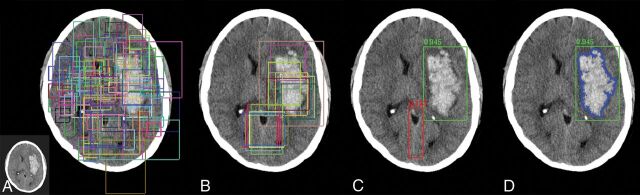
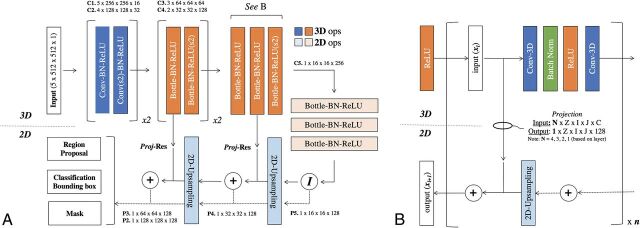
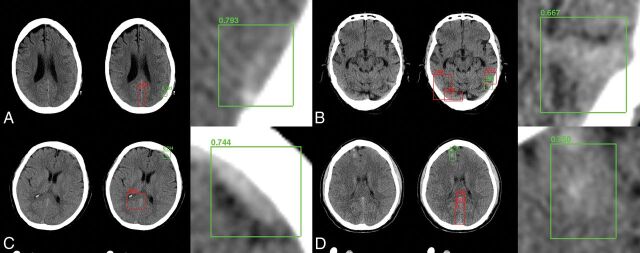
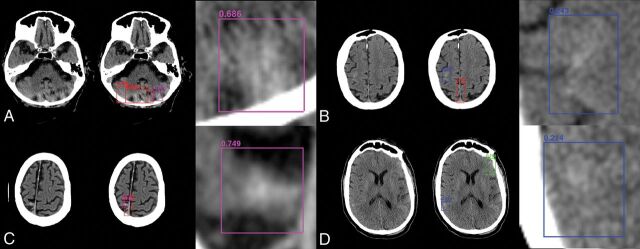
Materials and methods: This study was performed in 2 phases. First, a training cohort of all NCCTs acquired at a single institution between January 1, 2017, and July 31, 2017, was used to develop and cross-validate a custom hybrid 3D/2D mask ROI-based convolutional neural network architecture for hemorrhage evaluation. Second, the trained network was applied prospectively to all NCCTs ordered from the emergency department between February 1, 2018, and February 28, 2018, in an automated inference pipeline. Hemorrhage-detection accuracy, area under the curve, sensitivity, specificity, positive predictive value, and negative predictive value were assessed for full and balanced datasets and were further stratified by hemorrhage type and size. Quantification was assessed by the Dice score coefficient and the Pearson correlation.
Results: A 10,159-examination training cohort (512,598 images; 901/8.1% hemorrhages) and an 862-examination test cohort (23,668 images; 82/12% hemorrhages) were used in this study. Accuracy, area under the curve, sensitivity, specificity, positive predictive value, and negative-predictive value for hemorrhage detection were 0.975, 0.983, 0.971, 0.975, 0.793, and 0.997 on training cohort cross-validation and 0.970, 0.981, 0.951, 0.973, 0.829, and 0.993 for the prospective test set. Dice scores for intraparenchymal hemorrhage, epidural/subdural hemorrhage, and SAH were 0.931, 0.863, and 0.772, respectively.
Conclusions: A customized deep learning tool is accurate in the detection and quantification of hemorrhage on NCCT. Demonstrated high performance on prospective NCCTs ordered from the emergency department suggests the clinical viability of the proposed deep learning tool.
© 2018 by American Journal of Neuroradiology.
Figures
Comment in
-
Towards Reproducible Results: Validating CT Hemorrhage-Detection Algorithms on Standard Datasets.AJNR Am J Neuroradiol. 2018 Dec;39(12):E127. doi: 10.3174/ajnr.A5849. Epub 2018 Nov 29. AJNR Am J Neuroradiol. 2018. PMID: 30498018 Free PMC article. No abstract available.
-
Reply.AJNR Am J Neuroradiol. 2018 Dec;39(12):E128. doi: 10.3174/ajnr.A5913. Epub 2018 Nov 29. AJNR Am J Neuroradiol. 2018. PMID: 30498020 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources