

Recent Advances in the Management of Autosomal Dominant Polycystic Kidney Disease
- PMID: 30049849
- PMCID: PMC6237066
- DOI: 10.2215/CJN.03960318
Recent Advances in the Management of Autosomal Dominant Polycystic Kidney Disease
Abstract
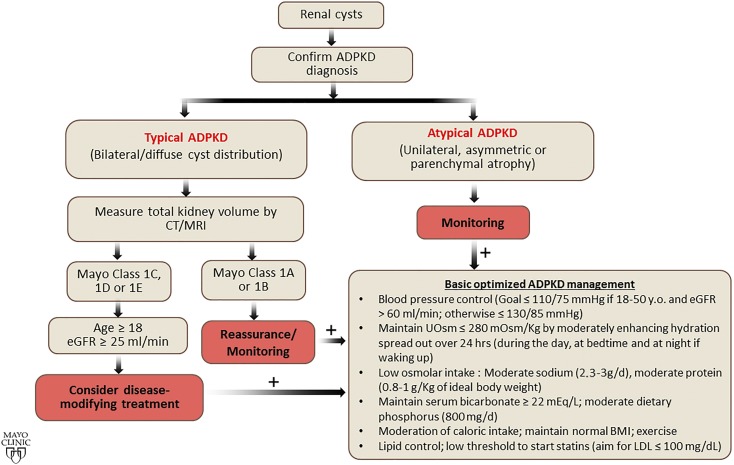
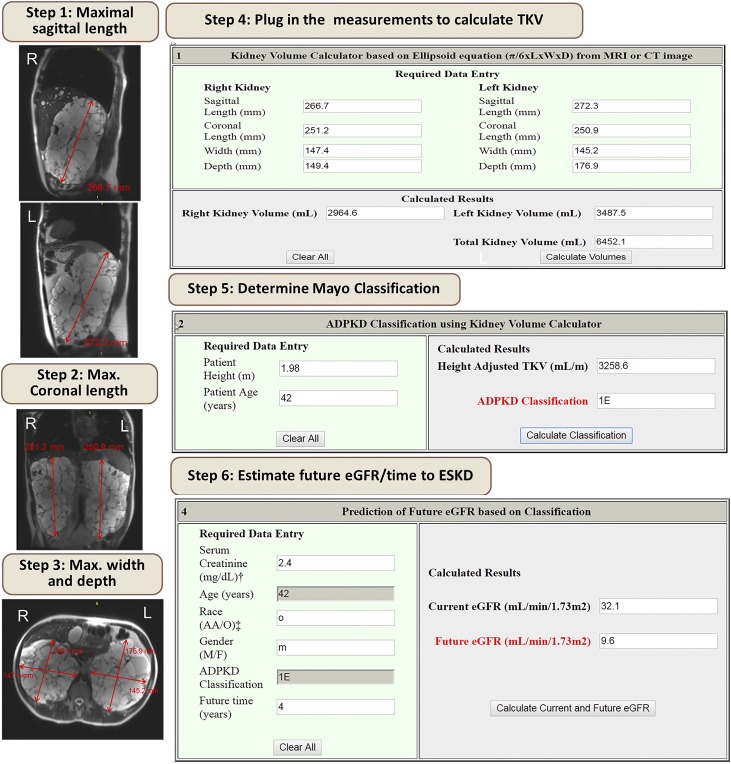
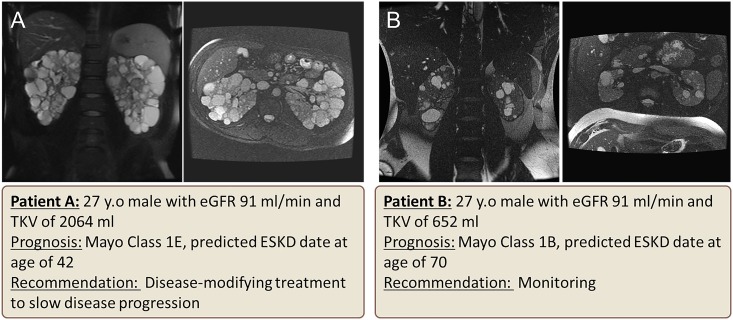
Autosomal dominant polycystic kidney disease (ADPKD), the most common monogenic cause of ESKD, is characterized by relentless development of kidney cysts, hypertension, and destruction of the kidney parenchyma. Over the past few years, major advancements in diagnosing, prognosticating, and understanding the pathogenesis and natural course of the disease have been made. Currently, no kidney disease is more suitable for nephron-protective strategies. Early nephrology referral and implementation of these strategies may have a substantial effect. Total kidney volume is a good prognostication marker and allows stratification of patients into slow or rapid progressing disease, with implications for their management. Measurement of total kidney volume, disease stratification, and prognostication are possible using readily available tools. Although some patients require only monitoring and basic optimized kidney protective measures, such as rigorous BP control and various lifestyle and dietary changes, others will benefit from disease-modifying treatments. Vasopressin V2 receptor antagonists, a likely disease-modifying treatment, has been approved in several countries and recently by the US Food and Drug Administration; other therapies, such as somatostatin analogs and other novel agents, are currently in clinical trials. The purpose of this article is to present our views on the optimal management to delay kidney disease progression in ADPKD.
Keywords: ADPKD; Antidiuretic Hormone Receptor Antagonists; Cysts; Dietary Sodium; Disease Progression; Kidney Failure, Chronic; Nephrons; Polycystic Kidney, Autosomal Dominant; Receptors, Vasopressin; Referral and Consultation; Somatostatin; United States Food and Drug Administration; blood pressure; hypertension; vasopressin.
Copyright © 2018 by the American Society of Nephrology.
Figures
References
-
- Grantham JJ, Torres VE, Chapman AB, Guay-Woodford LM, Bae KT, King BF Jr, Wetzel LH, Baumgarten DA, Kenney PJ, Harris PC, Klahr S, Bennett WM, Hirschman GN, Meyers CM, Zhang X, Zhu F, Miller JP; CRISP Investigators: Volume progression in polycystic kidney disease. N Engl J Med 354: 2122–2130, 2006 - PubMed
-
- Chapman AB, Bost JE, Torres VE, Guay-Woodford L, Bae KT, Landsittel D, Li J, King BF, Martin D, Wetzel LH, Lockhart ME, Harris PC, Moxey-Mims M, Flessner M, Bennett WM, Grantham JJ: Kidney volume and functional outcomes in autosomal dominant polycystic kidney disease. Clin J Am Soc Nephrol 7: 479–486, 2012 - PMC - PubMed
-
- Perrone RD, Mouksassi MS, Romero K, Czerwiec FS, Chapman AB, Gitomer BY, Torres VE, Miskulin DC, Broadbent S, Marier JF: Total kidney volume is a prognostic biomarker of renal function decline and progression to end-stage renal disease in patients with autosomal dominant polycystic kidney disease. Kidney Int Rep 2: 442–450, 2017 - PMC - PubMed
-
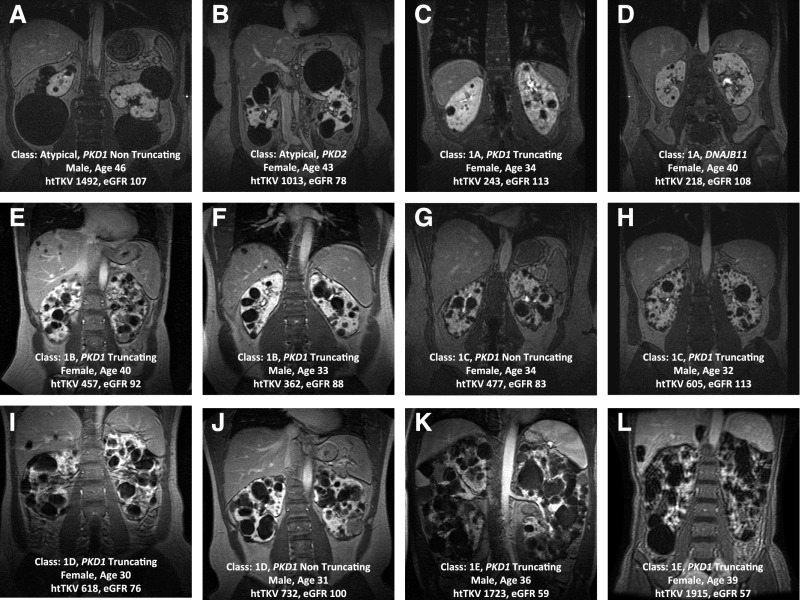
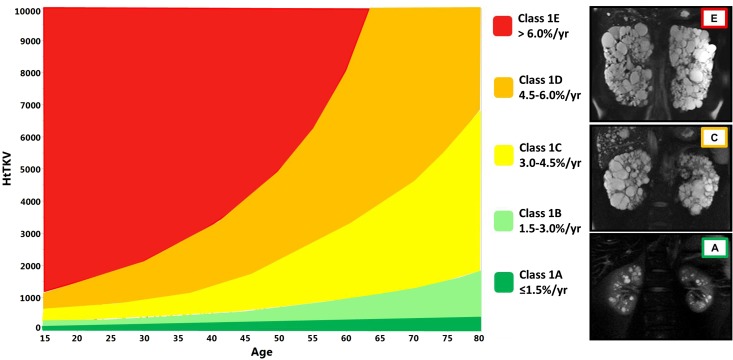
- Irazabal MV, Rangel LJ, Bergstralh EJ, Osborn SL, Harmon AJ, Sundsbak JL, Bae KT, Chapman AB, Grantham JJ, Mrug M, Hogan MC, El-Zoghby ZM, Harris PC, Erickson BJ, King BF, Torres VE; CRISP Investigators: Imaging classification of autosomal dominant polycystic kidney disease: A simple model for selecting patients for clinical trials. J Am Soc Nephrol 26: 160–172, 2015 - PMC - PubMed
-
- Kline TL, Korfiatis P, Edwards ME, Warner JD, Irazabal MV, King BF, Torres VE, Erickson BJ: Automatic total kidney volume measurement on follow-up magnetic resonance images to facilitate monitoring of autosomal dominant polycystic kidney disease progression. Nephrol Dial Transplant 31: 241–248, 2016 - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
