

Structural brain imaging in Alzheimer's disease and mild cognitive impairment: biomarker analysis and shared morphometry database
- PMID: 30050078
- PMCID: PMC6062561
- DOI: 10.1038/s41598-018-29295-9
Structural brain imaging in Alzheimer's disease and mild cognitive impairment: biomarker analysis and shared morphometry database
Abstract
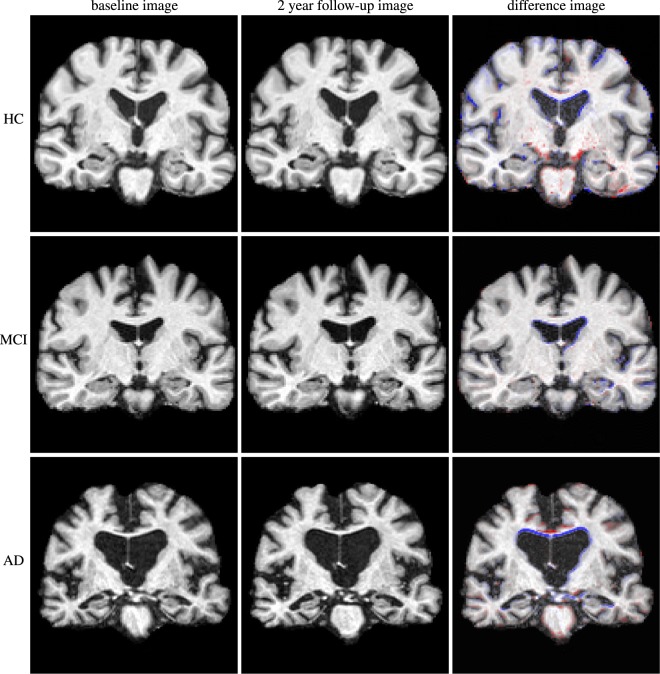
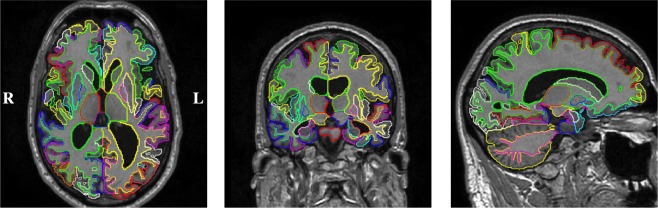
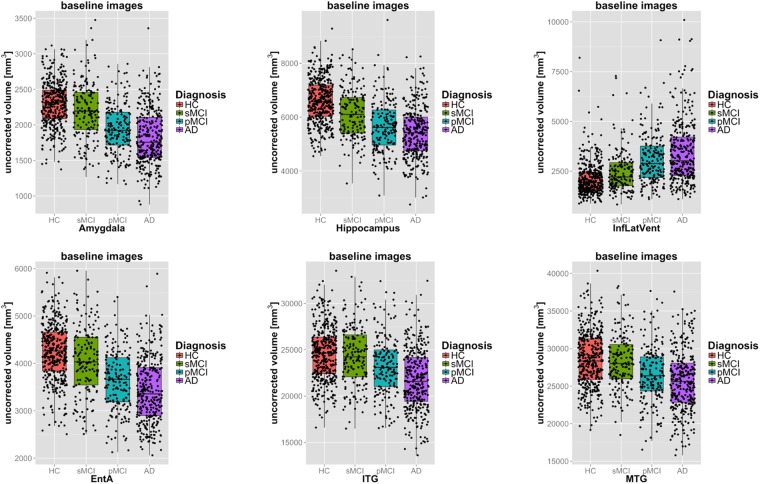
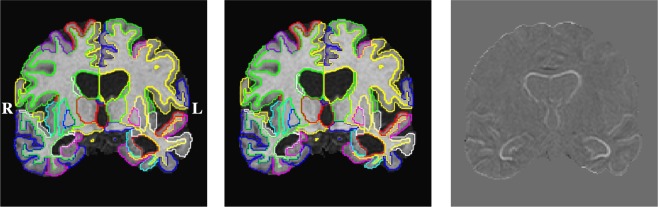
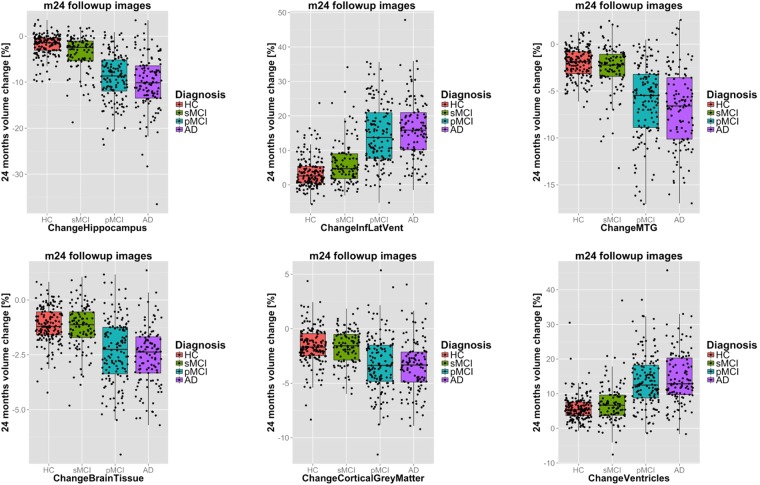
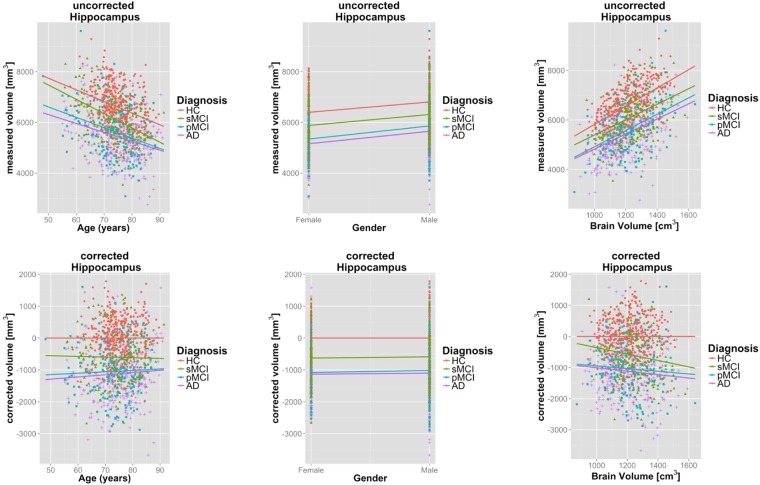
Magnetic resonance (MR) imaging is a powerful technique for non-invasive in-vivo imaging of the human brain. We employed a recently validated method for robust cross-sectional and longitudinal segmentation of MR brain images from the Alzheimer's Disease Neuroimaging Initiative (ADNI) cohort. Specifically, we segmented 5074 MR brain images into 138 anatomical regions and extracted time-point specific structural volumes and volume change during follow-up intervals of 12 or 24 months. We assessed the extracted biomarkers by determining their power to predict diagnostic classification and by comparing atrophy rates to published meta-studies. The approach enables comprehensive analysis of structural changes within the whole brain. The discriminative power of individual biomarkers (volumes/atrophy rates) is on par with results published by other groups. We publish all quality-checked brain masks, structural segmentations, and extracted biomarkers along with this article. We further share the methodology for brain extraction (pincram) and segmentation (MALPEM, MALPEM4D) as open source projects with the community. The identified biomarkers hold great potential for deeper analysis, and the validated methodology can readily be applied to other imaging cohorts.
Conflict of interest statement
C.L., A.S. and R.G. conducted this research while being employees of Imperial College London, U.K. (C.L., A.S., R.G.) and IXICO plc, U.K. (C.L., R.G.). D.R. is a co-founder and scientific advisor of IXICO plc, U.K., a provider of medical image analysis services. C.L. is currently employed by Imagen Technologies, Inc., N.Y., U.S.A. This does not alter thes’ adherence to Scientific Reports policies on sharing data and materials.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
