

A Consensus Statement on acromegaly therapeutic outcomes
- PMID: 30050156
- PMCID: PMC7136157
- DOI: 10.1038/s41574-018-0058-5
A Consensus Statement on acromegaly therapeutic outcomes
Abstract
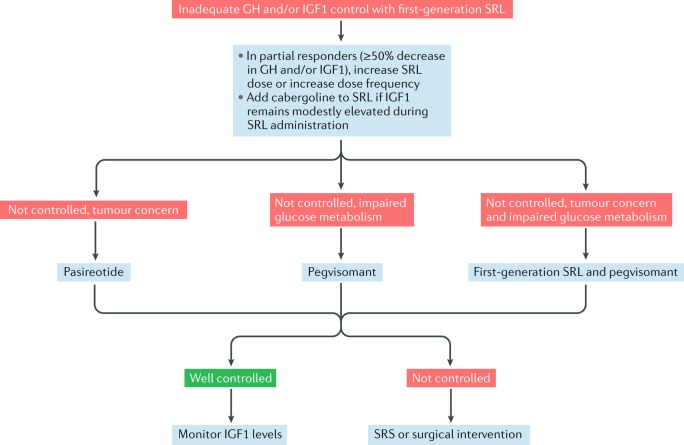
The 11th Acromegaly Consensus Conference in April 2017 was convened to update recommendations on therapeutic outcomes for patients with acromegaly. Consensus guidelines on the medical management of acromegaly were last published in 2014; since then, new pharmacological agents have been developed and new approaches to treatment sequencing have been considered. Thirty-seven experts in the management of patients with acromegaly reviewed the current literature and assessed changes in drug approvals, clinical practice standards and clinical opinion. They considered current treatment outcome goals with a focus on the impact of current and emerging somatostatin receptor ligands, growth hormone receptor antagonists and dopamine agonists on biochemical, clinical, tumour mass and surgical outcomes. The participants discussed factors that would determine pharmacological choices as well as the proposed place of each agent in the guidelines. We present consensus recommendations highlighting how acromegaly management could be optimized in clinical practice.
Conflict of interest statement
S.M. is a consultant for Chiasma, Ionis, Ipsen and Strongbridge Pharma and receives research grants from Pfizer. M.D.B. is a consultant for Ipsen and Novartis, a speakers bureau member for Ipsen and has received research grants from Novartis. P.C. has received unrestricted research and educational grants from Ipsen, Novartis and Pfizer as head of the Department of Endocrinology and Reproductive Diseases, Hôpitaux Universitaires Paris-Sud,has served as investigator for clinical trials funded by Antisense, Chiasma, Ipsen, Italpharmaco, Novartis and Pfizer and is a consultant for Ipsen, Novartis and Pfizer. All fees and honoraria are paid to his institution. A.K. is a consultant for Chiasma and Crinetics and has received research grants from Ipsen. F.F.C. is a speakers bureau member for Pfizer and has received research grants from Ipsen and Pfizer. C.J.S. is an advisory board member for Pfizer and a speakers bureau member for Pfizer and Ipsen. A.L. is a consultant for Ipsen and Novartis, a speakers bureau member for Ipsen, Novartis and Pfizer and has received research grants from Pfizer. D.R.C. is a consultant for Crinetics, Ipsen and Pfizer. A.G. is a consultant for Ipsen, Novartis and Pfizer. J.A.H.W. declares no competing interests.
Figures
References
-
- Melmed S. Medical progress: Acromegaly. N. Engl. J. Med. 2006;355:2558–2573. - PubMed
-
- Colao A, Ferone D, Marzullo P, Lombardi G. Systemic complications of acromegaly: epidemiology, pathogenesis, and management. Endocr. Rev. 2004;25:102–152. - PubMed
-
- Giustina A, et al. Expert consensus document: A consensus on the medical treatment of acromegaly. Nat. Rev. Endocrinol. 2014;10:243–248. - PubMed
-
- Katznelson L, et al. Acromegaly: an endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2014;99:3933–3951. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
