

Extrapulmonary neoplasms in lung cancer screening
- PMID: 30050774
- PMCID: PMC6037975
- DOI: 10.21037/tlcr.2018.06.05
Extrapulmonary neoplasms in lung cancer screening
Abstract
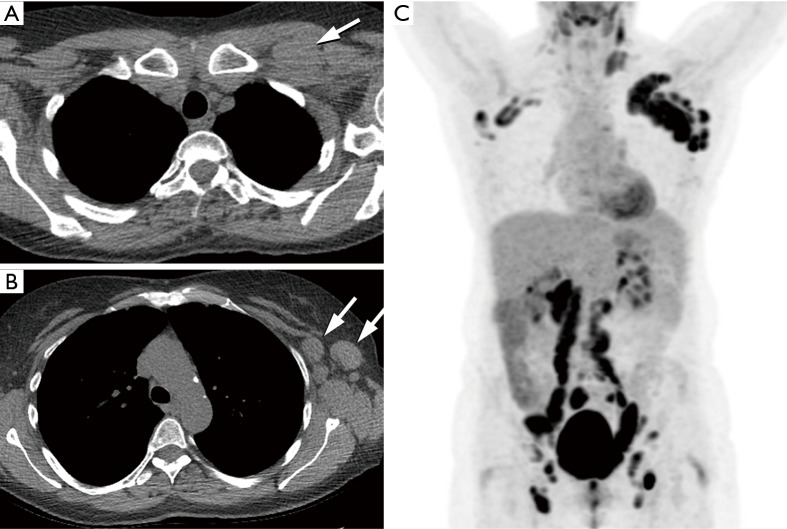
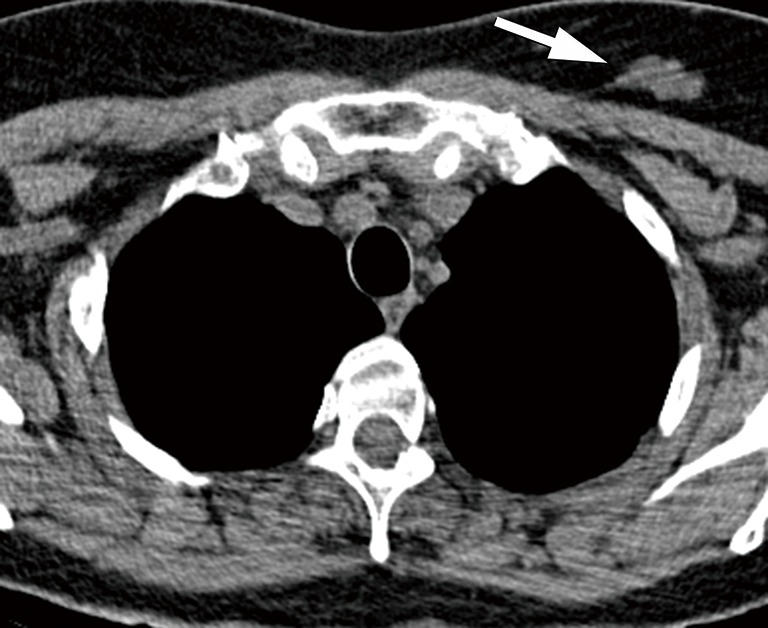
A significant reduction in lung cancer specific mortality rate was demonstrated by the National Lung Screening Trial (NLST) in participants who had annual low-dose computed tomography (LDCT) screening. In addition to early detection of lung cancer, lung cancer screening (LCS) provides an opportunity to detect cardiovascular disease, pulmonary disease (such as chronic obstructive pulmonary disease and interstitial lung disease), and extrapulmonary neoplasms, such as thyroid, breast, kidney, liver, esophageal, pancreatic and mediastinal tumors. Considering the fact that 22.3% of the certified deaths in the computed tomography (CT) arm of the NLST trial were due to extrapulmonary malignancies, compared to 22.9% of deaths from lung cancer, it is possible that early diagnosis and treatment of clinically significant incidental findings may further decrease morbidity and mortality in screening participants. In this article we review prevalence, clinical relevance and management of incidentally detected extrapulmonary malignancies.
Keywords: Lung cancer; computed tomography (CT); incidental findings (IFs); low-dose computed tomography (LDCT); neoplasm; screening.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare
Figures





References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources