

Centralized Waiting Lists for Unattached Patients in Primary Care: Learning from an Intervention Implemented in Seven Canadian Provinces
- PMID: 30052190
- PMCID: PMC6044259
- DOI: 10.12927/hcpol.2018.25555
Centralized Waiting Lists for Unattached Patients in Primary Care: Learning from an Intervention Implemented in Seven Canadian Provinces
Erratum in
-
Corrigendum.Healthc Policy. 2018 Aug;14(1):10. doi: 10.12927/hcpol.2018.25553. Healthc Policy. 2018. PMID: 31329750 Free PMC article.
Abstract
Introduction: Centralized waiting lists (CWLs) are one solution to reduce the problematic number of patients without a regular primary care provider. This article describes different models of CWLs for unattached patients implemented in seven Canadian provinces and identifies common issues in the implementation of these CWLs.
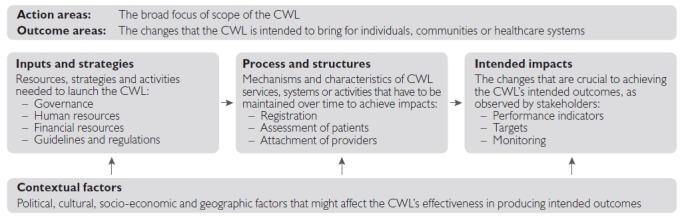
Methods: Logic models of each province's intervention were built after a grey literature review, 42 semi-structured interviews and a validation process with key stakeholders were performed.
Results: Our analysis across provinces showed variability and common features in the design of CWLs such as same main objective to attach patients to a primary care provider; implementation as a province-wide program with the exception of British Columbia; management at a regional level in most provinces; voluntary participation for providers except in two provinces where it was mandatory for providers to attach CWL patients; fairly similar registration process across the provinces; some forms of prioritization of patients either using simple criteria or assessing for vulnerability was performed in most provinces except New Brunswick.
Conclusion: Despite their differences in design, CWLs implemented in seven Canadian provinces face common issues and challenges regarding provider capacity to address the demand for attachment, barriers to the attachment of more vulnerable and complex patients as well as non-standardized approaches to evaluating their effectiveness. Sharing experiences across provinces as CWLs were being implemented would have fostered learning and could have helped avoid facing similar challenges.
Introduction:: Les listes d'attente centralisées (LAC) constituent une solution afin de réduire les problématiques reliées au taux de patients sans affiliation à un professionnel de première ligne. Cet article décrit divers modèles de LAC pour les patients non-affiliés qui ont été implantés dans sept provinces canadiennes et recense les enjeux communs liés à leur mise en œuvre.
Méthode:: Des modèles logiques pour chacune des interventions provinciales ont été élaborés suite à une revue de la littérature grise, à 42 entrevues semi-dirigées et à un processus de validation auprès d'acteurs concernés.
Résultats:: Notre analyse montre une variabilité et des caractéristiques communes dans la conception des LAC, notamment un même objectif principal visant la prise en charge des patients par un professionnel de première ligne; la mise en œuvre d'un programme pour l'ensemble de la province, à l'exception de la Colombie-Britannique; la gestion au niveau régional dans la plupart des provinces; la participation volontaire des professionnels, sauf dans deux provinces où ils ont l'obligation de prendre en charge les patients inscrits à la LAC; des processus d'inscription plutôt similaires d'une province à l'autre; une certaine forme de priorisation des patients, soit à l'aide de critères simples ou en évaluant leur vulnérabilité, et ce, dans la plupart des provinces sauf au Nouveau-Brunswick.
Conclusion:: Malgré les différences dans la conception, les LAC mis en œuvre dans sept provinces canadiennes font face à des enjeux et défis communs quant à la capacité de traiter les demandes de prise en charge, quant aux obstacles pour la prise en charge des patients plus vulnérables et dont l'état est complexe, et quant à la non standardisation des processus pour l'évaluation de l'efficacité. Le partage de l'expérience entre les provinces au moment de la mise en œuvre des LAC aurait favorisé l'apprentissage et aurait permis d'éviter de rencontrer des défis similaires.
© 2018 Longwoods Publishing.
References
-
- Breton M., Green M., Kreindler S., Sutherland J., Jbilou J., Wong S.T. et al. 2017. “A Comparative Analysis of Centralized Waiting Lists for Patients without a Primary Care Provider Implemented in Six Canadian Provinces: Study Protocol.” BMC Health Services Research 17(1): 60. 10.1186/s12913-017-2007-8. - PMC - PubMed
-
- Brousselle A., Champagne F. 2011. “Program Theory Evaluation: Logic Analysis.” Evaluation and Program Planning 34: 69–78. - PubMed
-
- Burge F., Lawson B., Johnston G. 2003. “Family Physician Continuity of Care and Emergency Department Use in End-of-Life Cancer Care.” Medical Care 41(8): 992–1001. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical