

Comparison of continuous thoracic epidural analgesia with bilateral erector spinae plane block for perioperative pain management in cardiac surgery
- PMID: 30052229
- PMCID: PMC6078032
- DOI: 10.4103/aca.ACA_16_18
Comparison of continuous thoracic epidural analgesia with bilateral erector spinae plane block for perioperative pain management in cardiac surgery
Abstract
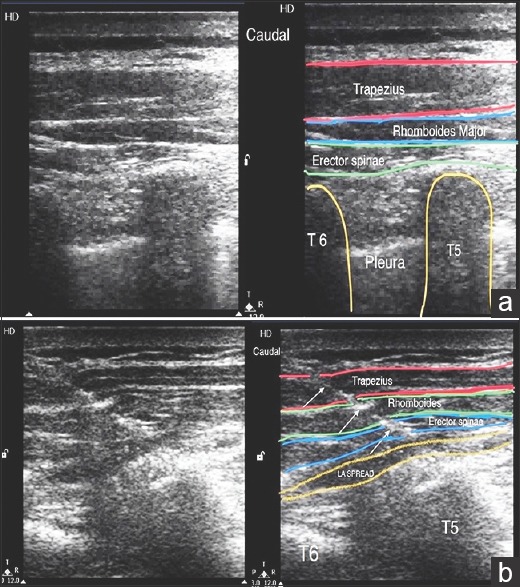
Objective: Continuous thoracic epidural analgesia (TEA) is compared with erector spinae plane (ESP) block for the perioperative pain management in patients undergoing cardiac surgery for the quality of analgesia, incentive spirometry, ventilator duration, and intensive care unit (ICU) duration.
Methodology: A prospective, randomized comparative clinical study was conducted. A total of 50 patients were enrolled, who were randomized to either Group A: TEA (n = 25) or Group B: ESP block (n = 25). Visual analog scale (VAS) was recorded in both the groups during rest and cough at the various time intervals postextubation. Both the groups were also compared for incentive spirometry, ventilator, and ICU duration. Statistical analysis was performed using the independent Student's t-test. A value of P < 0.05 was considered statistically significant.
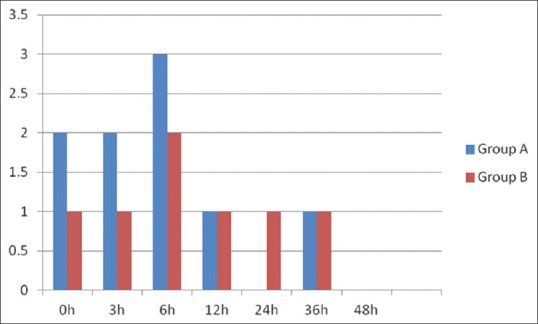
Results: c: omparable VAS scores were revealed at 0 h, 3 h, 6 h, and 12 h (P > 0.05) at rest and during cough in both the groups. Group A had a statistically significant VAS score than Group B (P ≤ 0.05) at 24 h, 36 h, and 48 h but mean VAS in either of the Group was ≤4 both at rest and during cough. Incentive spirometry, ventilator, and ICU duration were comparable between the groups.
Conclusion: ESP block is easy to perform and can serve as a promising alternative to TEA in optimal perioperative pain management in cardiac surgery.
Keywords: Erector spinae plane block; thoracic epidural analgesia; visual analog scale.
Conflict of interest statement
There are no conflicts of interest
Figures
References
-
- Cogan J. Pain management after cardiac surgery. Semin Cardiothorac Vasc Anesth. 2010;14:201–4. - PubMed
-
- American Society of Anesthesiologists Task Force on Acute Pain Management. Practice guidelines for acute pain management in the perioperative setting: An updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology. 2012;116:248–73. - PubMed
-
- Dhole S, Mehta Y, Saxena H, Juneja R, Trehan N. Comparison of continuous thoracic epidural and paravertebral blocks for postoperative analgesia after minimally invasive direct coronary artery bypass surgery. J Cardiothorac Vasc Anesth. 2001;15:288–92. - PubMed
-
- Mehta Y, Arora D, Sharma KK, Mishra Y, Wasir H, Trehan N, et al. Comparison of continuous thoracic epidural and paravertebral block for postoperative analgesia after robotic-assisted coronary artery bypass surgery. Ann Card Anaesth. 2008;11:91–6. - PubMed
-
- Cantó M, Sánchez MJ, Casas MA, Bataller ML. Bilateral paravertebral blockade for conventional cardiac surgery. Anaesthesia. 2003;58:365–70. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical