

Pharmacometabolomics Reveals Irinotecan Mechanism of Action in Cancer Patients
- PMID: 30052267
- PMCID: PMC6857457
- DOI: 10.1002/jcph.1275
Pharmacometabolomics Reveals Irinotecan Mechanism of Action in Cancer Patients
Abstract
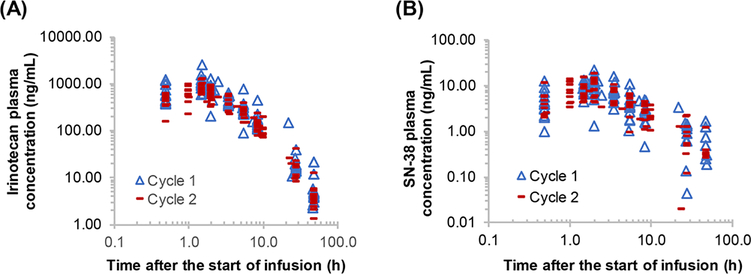
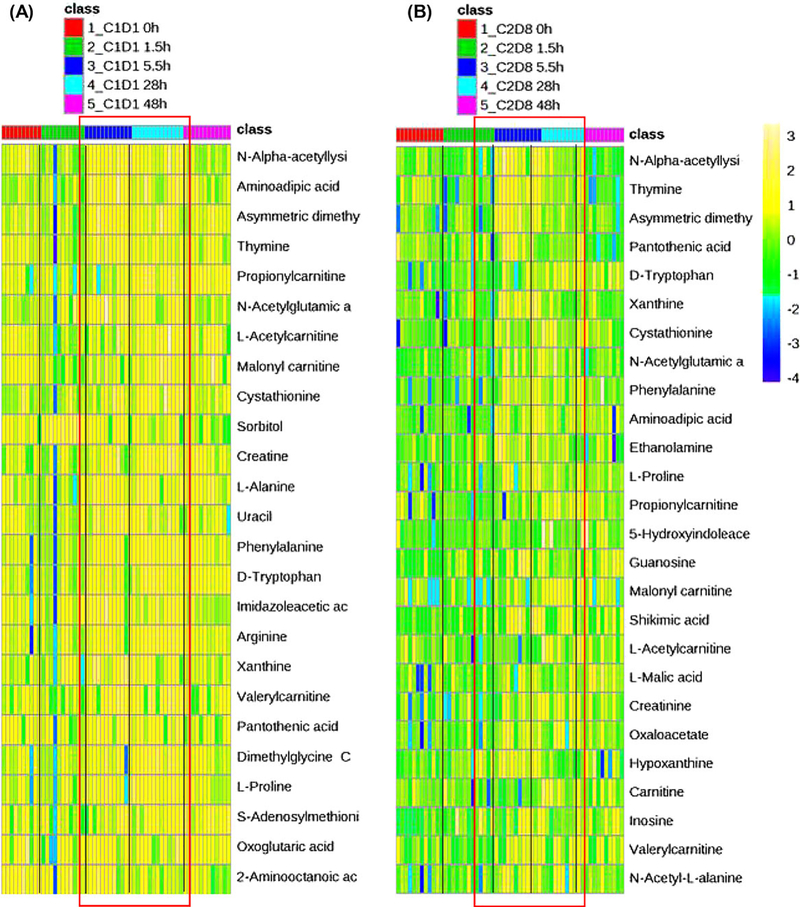
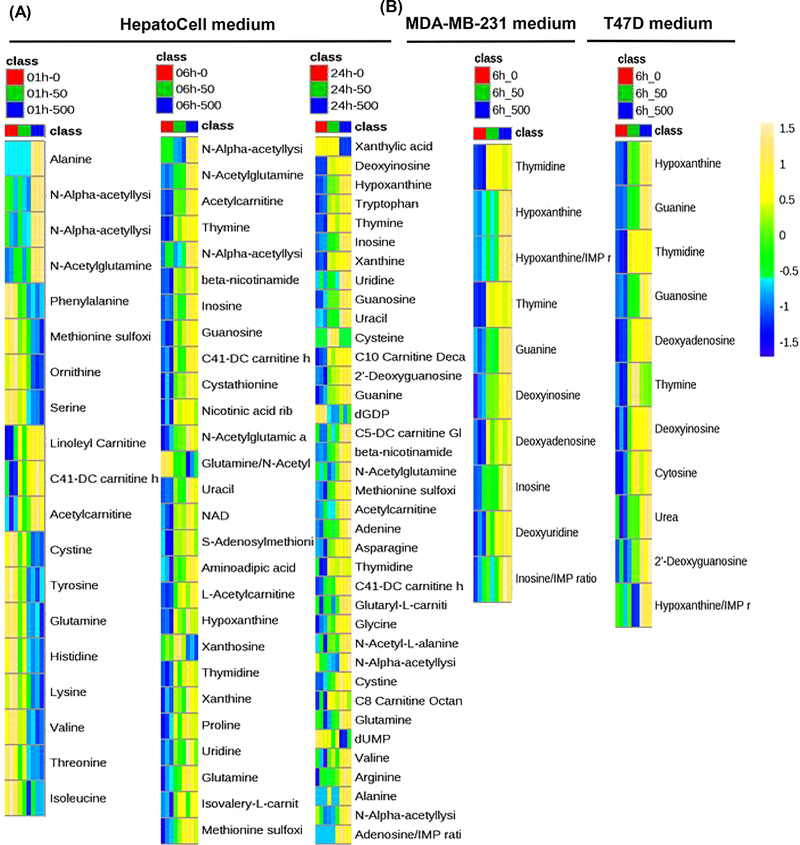
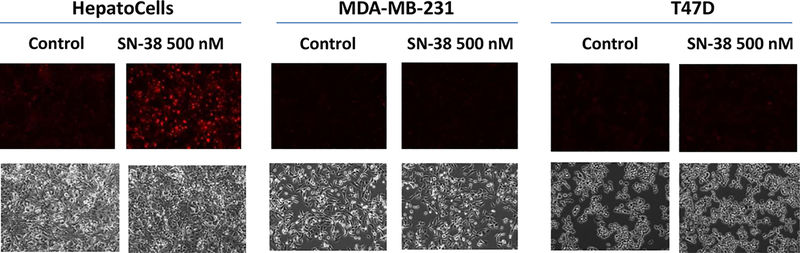
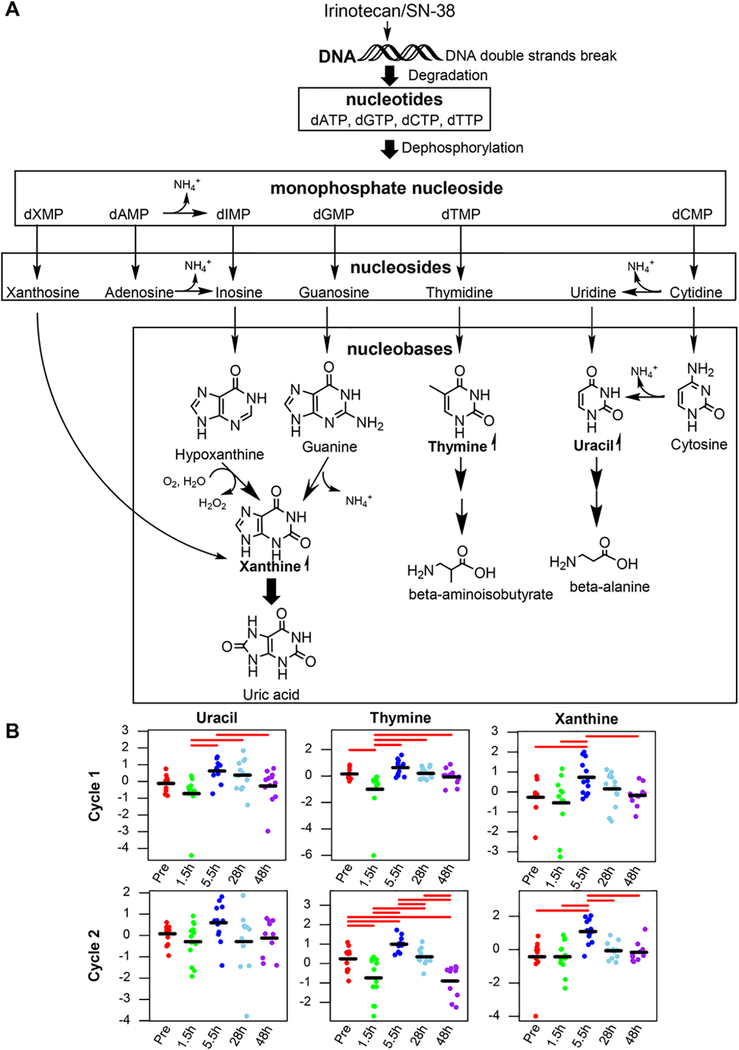
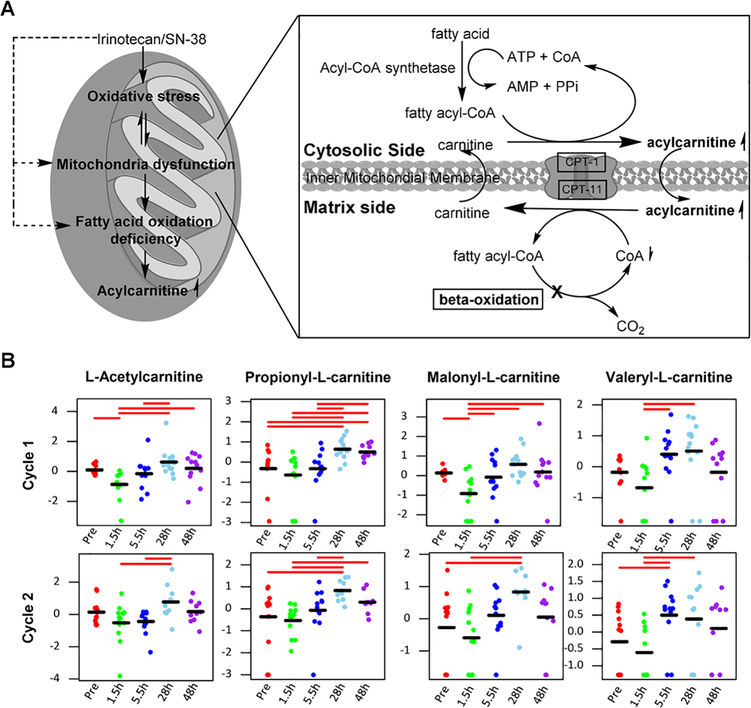
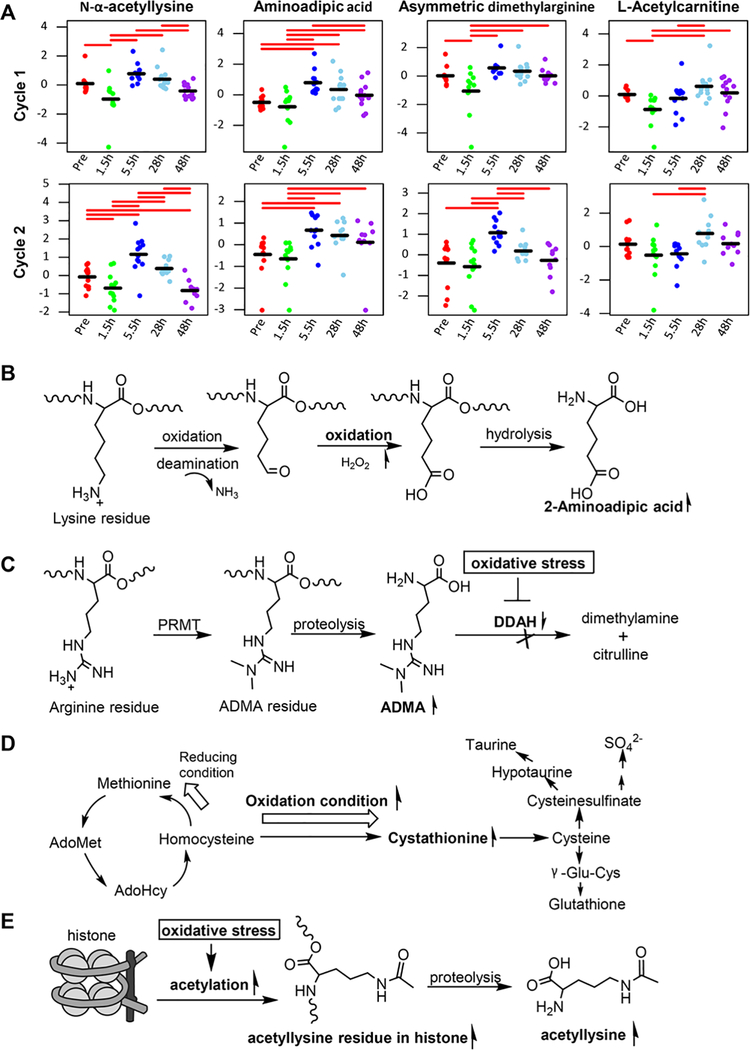
The purpose of this study was to identify early circulating metabolite changes implicated in the mechanism of action of irinotecan, a DNA topoisomerase I inhibitor, in cancer patients. A liquid chromatography-tandem mass spectrometry-based targeted metabolomic platform capable of measuring 254 endogenous metabolites was applied to profile circulating metabolites in plasma samples collected pre- and post-irinotecan treatment from 13 cancer patients. To gain further mechanistic insights, metabolic profiling was also performed for the culture medium of human primary hepatocytes (HepatoCells) and 2 cancer cell lines on exposure to SN-38 (an active metabolite of irinotecan). Intracellular reactive oxygen species (ROS) was detected by dihydroethidium assay. Irinotecan induced a global metabolic change in patient plasma, as represented by elevations of circulating purine/pyrimidine nucleobases, acylcarnitines, and specific amino acid metabolites. The plasma metabolic signature was well replicated in HepatoCells medium on SN-38 exposure, whereas in cancer cell medium SN-38 induced accumulation of pyrimidine/purine nucleosides and nucleobases while having no impact on acylcarnitines and amino acid metabolites. SN-38 induced ROS in HepatoCells, but not in cancer cells. Distinct metabolite signatures of SN-38 exposure in HepatoCells medium and cancer cell medium revealed different mechanisms of drug action on hepatocytes and cancer cells. Elevations in circulating purine/pyrimidine nucleobases may stem from nucleotide degradation following irinotecan-induced DNA double-strand breaks. Accumulations of circulating acylcarnitines and specific amino acid metabolites may reflect, at least in part, irinotecan-induced mitochondrial dysfunction and oxidative stress in the liver. The plasma metabolic signature of irinotecan exposure provides early insights into irinotecan mechanism of action in patients.
Keywords: DNA double-strand break; irinotecan; metabolomics; mitochondrial dysfunction; oxidative stress; steatohepatitis.
© 2018, The American College of Clinical Pharmacology.
Conflict of interest statement
Declaration of Conflicting Interests
The authors declare that there are no conflicts of interest.
Figures
References
-
- Saltz LB, Cox JV, Blanke C, et al. Irinotecan plus fluorouracil and leucovorin for metastatic colorectal cancer. Irinotecan Study Group. N Engl J Med. 2000;343(13):905–914. - PubMed
-
- Punt CJ, Koopman M. Capecitabine and irinotecan as first-line treatment of advanced colorectal cancer. J Clin Oncol. 2008;26(11):1907–1908; author reply 1908–1909. - PubMed
-
- Mathijssen RH, Loos WJ, Verweij J, Sparreboom A. Pharmacology of topoisomerase I inhibitors irinotecan (CPT-11) and topotecan. Curr Cancer Drug Targets. 2002;2(2):103–123. - PubMed
-
- Liu LF, Desai SD, Li TK, Mao Y, Sun M, Sim SP. Mechanism of action of camptothecin. Ann N Y Acad Sci. 2000;922:1–10. - PubMed
-
- Vauthey JN, Pawlik TM, Ribero D, et al. Chemotherapy regimen predicts steatohepatitis and an increase in 90-day mortality after surgery for hepatic colorectal metastases. J Clin Oncol. 2006;24(13):2065–2072. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
