

Trends in Bone Marrow Sampling and Core Biopsy Specimen Adequacy in the United States and Canada: A Multicenter Study
- PMID: 30052721
- PMCID: PMC6166687
- DOI: 10.1093/ajcp/aqy066
Trends in Bone Marrow Sampling and Core Biopsy Specimen Adequacy in the United States and Canada: A Multicenter Study
Abstract
Objectives: To assess bone marrow (BM) sampling in academic medical centers.
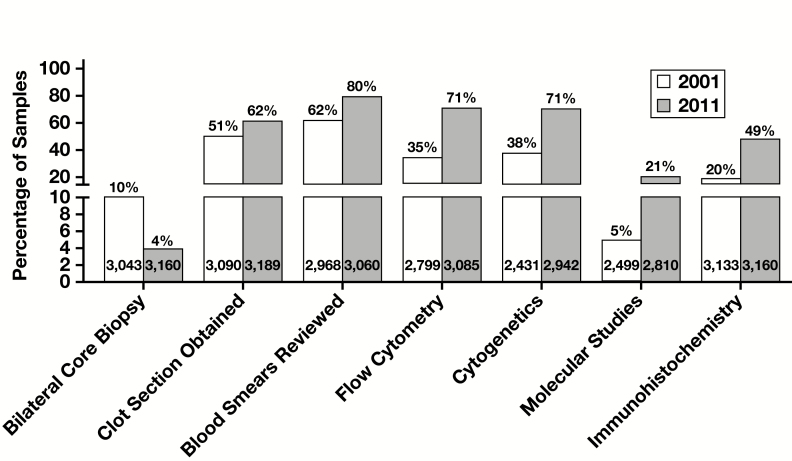
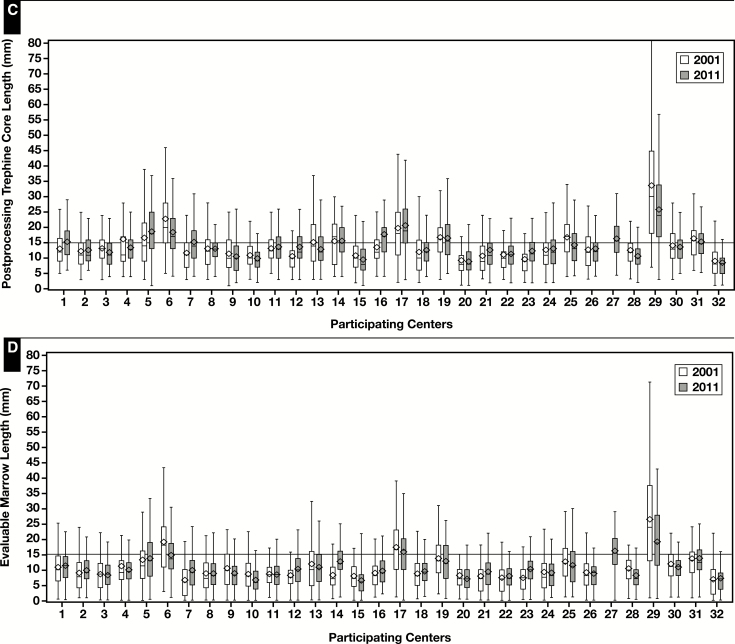
Methods: Data from 6,374 BM samples obtained in 32 centers in 2001 and 2011, including core length (CL), were analyzed.
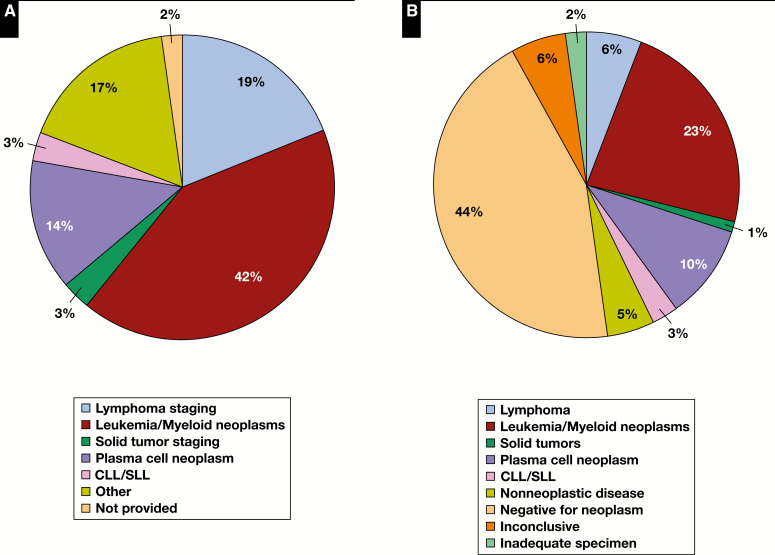
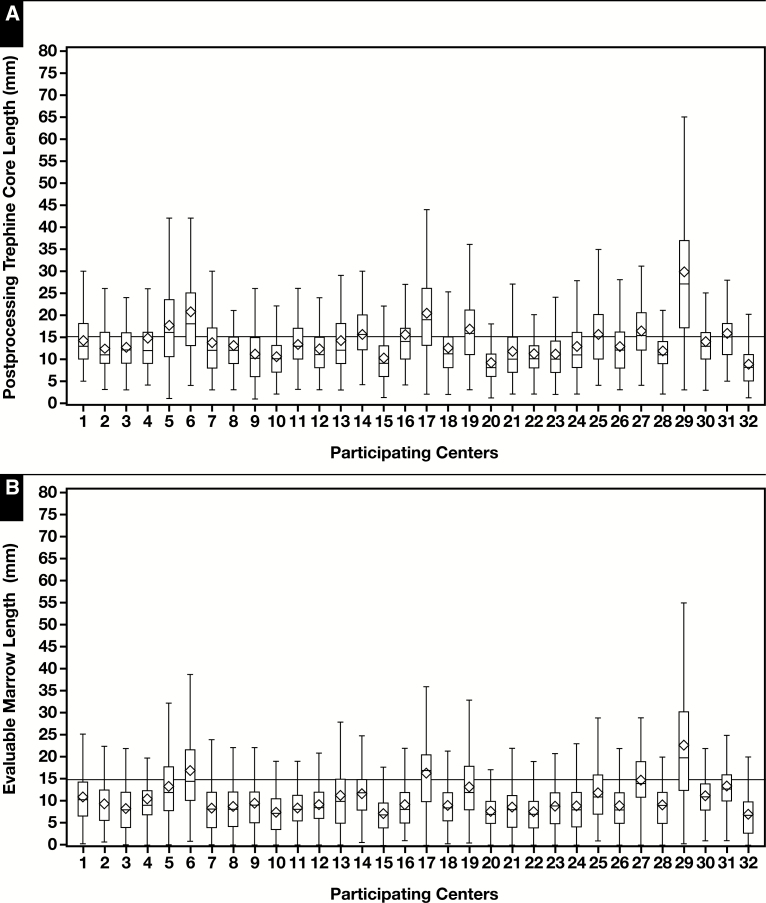
Results: BM included a biopsy (BMB; 93%) specimen, aspirate (BMA; 92%) specimen, or both (83%). The median (SD) CL was 12 (8.5) mm, and evaluable marrow was 9 (7.6) mm. Tissue contraction due to processing was 15%. BMB specimens were longer in adults younger than 60 years, men, and bilateral, staging, and baseline samples. Only 4% of BMB and 2% of BMB/BMA samples were deemed inadequate for diagnosis. BM for plasma cell dyscrasias, nonphysician operators, and ancillary studies usage increased, while bilateral sampling decreased over the decade. BM-related quality assurance programs are infrequent.
Conclusions: CL is shorter than recommended and varies with patient age and sex, clinical circumstances, and center experience. While pathologists render diagnoses on most cases irrespective of CL, BMB yield improvement is desirable.
Figures
References
-
- Lee SH, Erber WN, Porwit A, et al. ; International Council for Standardization in Hematology. ICSH guidelines for the standardization of bone marrow specimens and reports. Int J Lab Hematol. 2008;30:349-364. - PubMed
-
- Arber D, Hasserjian RP. Introduction and overview of the classification of myeloid neoplasms. In: Swerdlow SH, Campo E, Harris NL, et al. eds. WHO Classification of Tumours. Lyon, France: IARC; 2017:16-27.
-
- NCCN Clinical Practice Guidelines in Oncology. B-cell lymphomas. Version 3.2018. https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf. Accessed April 13, 2018.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
