

Difficult-to-Treat Resistance in Gram-negative Bacteremia at 173 US Hospitals: Retrospective Cohort Analysis of Prevalence, Predictors, and Outcome of Resistance to All First-line Agents
- PMID: 30052813
- PMCID: PMC6260171
- DOI: 10.1093/cid/ciy378
Difficult-to-Treat Resistance in Gram-negative Bacteremia at 173 US Hospitals: Retrospective Cohort Analysis of Prevalence, Predictors, and Outcome of Resistance to All First-line Agents
Abstract
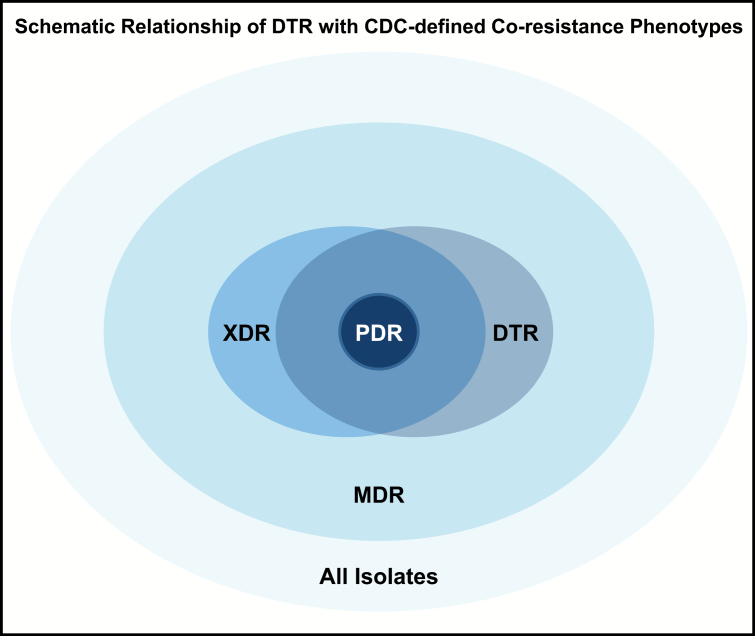
Background: Resistance to all first-line antibiotics necessitates the use of less effective or more toxic "reserve" agents. Gram-negative bloodstream infections (GNBSIs) harboring such difficult-to-treat resistance (DTR) may have higher mortality than phenotypes that allow for ≥1 active first-line antibiotic.
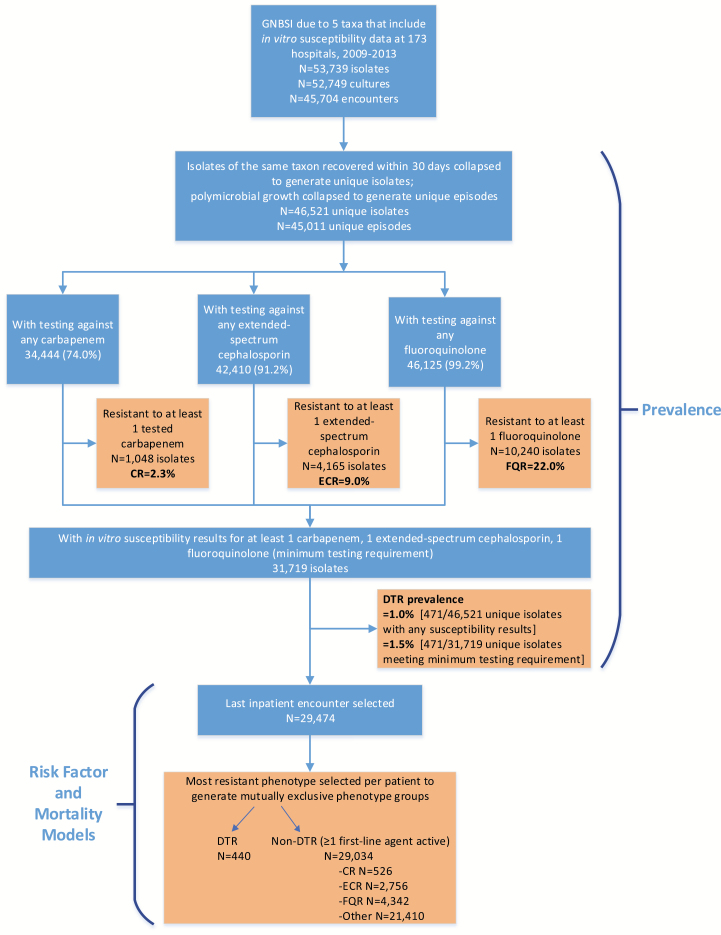
Methods: The Premier Database was analyzed for inpatients with select GNBSIs. DTR was defined as intermediate/resistant in vitro to all ß-lactam categories, including carbapenems and fluoroquinolones. Prevalence and aminoglycoside resistance of DTR episodes were compared with carbapenem-resistant, extended-spectrum cephalosporin-resistant, and fluoroquinolone-resistant episodes using CDC definitions. Predictors of DTR were identified. The adjusted relative risk (aRR) of mortality was examined for DTR, CDC-defined phenotypes susceptible to ≥1 first-line agent, and graded loss of active categories.
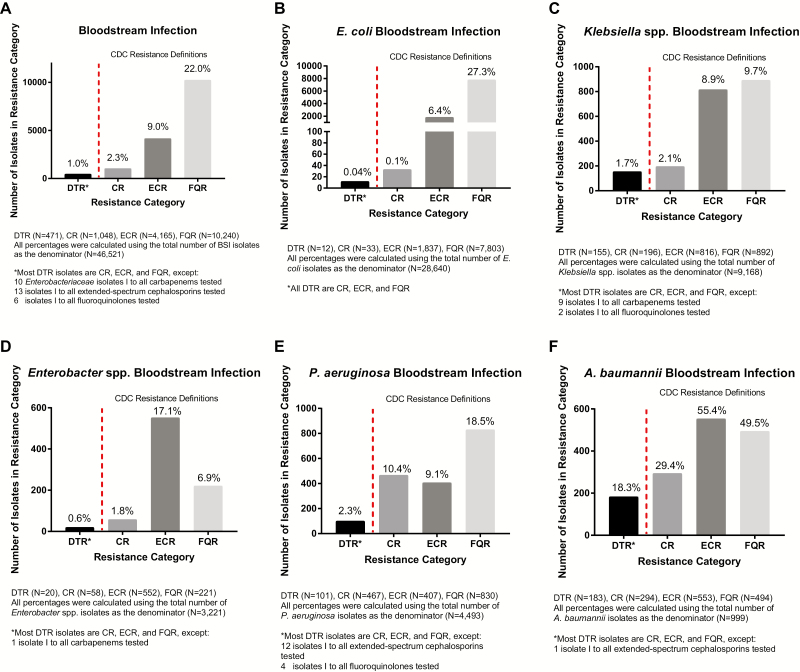
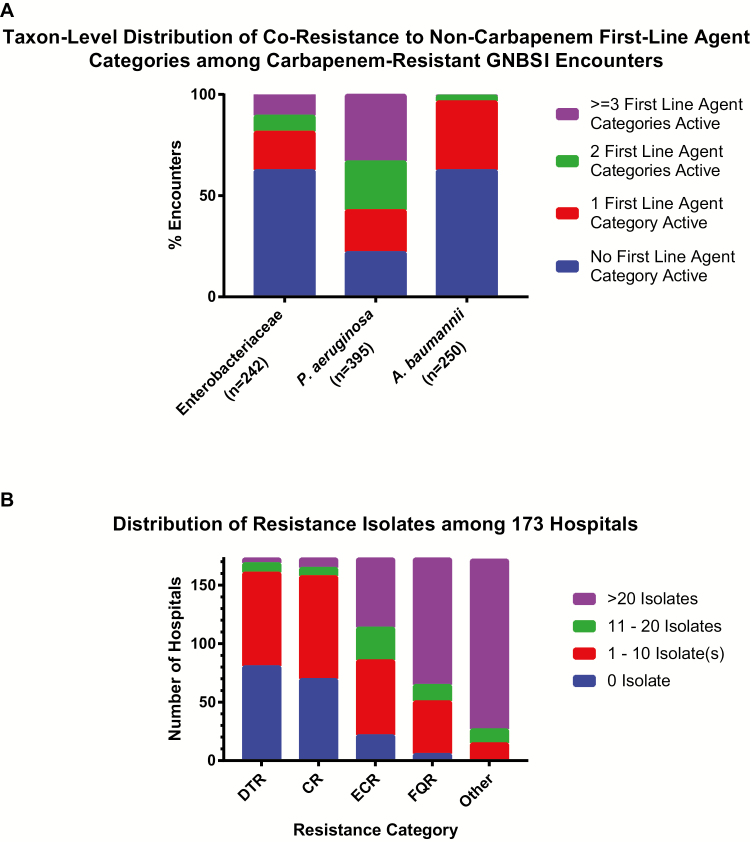
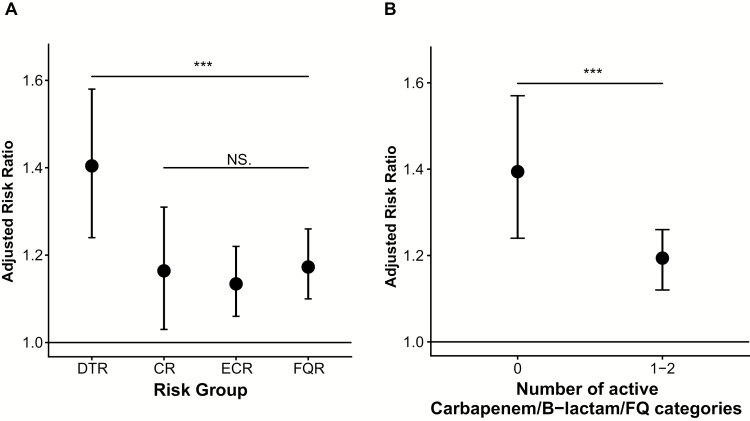
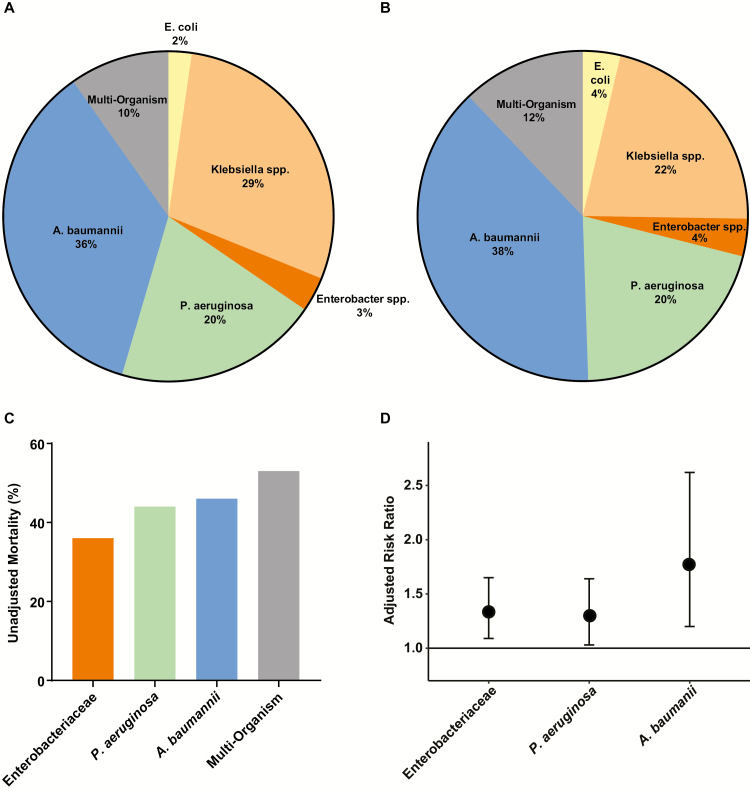
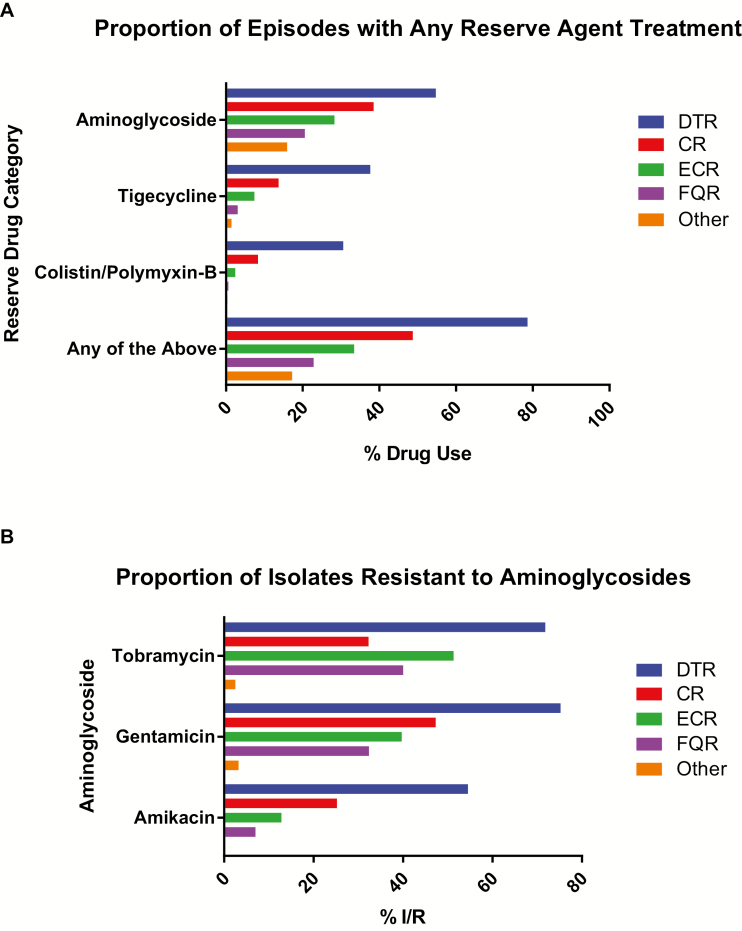
Results: Between 2009-2013, 471 (1%) of 45011 GNBSI episodes at 92 (53.2%) of 173 hospitals exhibited DTR, ranging from 0.04% for Escherichia coli to 18.4% for Acinetobacter baumannii. Among patients with DTR, 79% received parenteral aminoglycosides, tigecycline, or colistin/polymyxin-B; resistance to all aminoglycosides occurred in 33%. Predictors of DTR included urban healthcare and higher baseline illness. Crude mortality for GNBSIs with DTR was 43%; aRR was higher for DTR than for carbapenem-resistant (1.2; 95% confidence interval, 1.0-1.4; P = .02), extended-spectrum cephalosporin-resistant (1.2; 1.1-1.4; P = .001), or fluoroquinolone-resistant (1.2; 1.0-1.4; P = .008) infections. The mortality aRR increased 20% per graded loss of active first-line categories, from 3-5 to 1-2 to 0.
Conclusion: Nonsusceptibility to first-line antibiotics is associated with decreased survival in GNBSIs. DTR is a simple bedside prognostic measure of treatment-limiting coresistance.
Figures
Comment in
-
The Paradigm of the Shadoks and Antibiotic Resistance.Clin Infect Dis. 2019 Oct 15;69(9):1641. doi: 10.1093/cid/ciz183. Clin Infect Dis. 2019. PMID: 30838399 No abstract available.
-
Difficult to Treat: Do We Need a New Definition?Clin Infect Dis. 2019 Oct 15;69(9):1641-1642. doi: 10.1093/cid/ciz184. Clin Infect Dis. 2019. PMID: 30838418 No abstract available.
-
Reply to Raoult and Rolain, and to Echols and Tillotson.Clin Infect Dis. 2019 Oct 15;69(9):1642-1644. doi: 10.1093/cid/ciz186. Clin Infect Dis. 2019. PMID: 30839092 Free PMC article. No abstract available.
References
-
- Centers for Disease Control and Prevention. Antibiotic resistance threats in the United States, 2013. Available at: http://www.cdc.gov/drugresistance/pdf/ar-threats-2013–508.pdf. Accessed 20 October 2017.
-
- O’Neill J. Antimicrobial resistance: tackling a crisis for the health and wealth of nations. In: Review on antimicrobial resistance. Antimicrobial resistance: tackling a crisis for the health and wealth of nations. 2014. Available at: https://amr-review.org/sites/default/files/AMR%20Review%20Paper%20-%20Ta.... Accessed 20 June 2018.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
