

Lewy Body Pathology and Chronic Traumatic Encephalopathy Associated With Contact Sports
- PMID: 30053297
- PMCID: PMC6097837
- DOI: 10.1093/jnen/nly065
Lewy Body Pathology and Chronic Traumatic Encephalopathy Associated With Contact Sports
Abstract
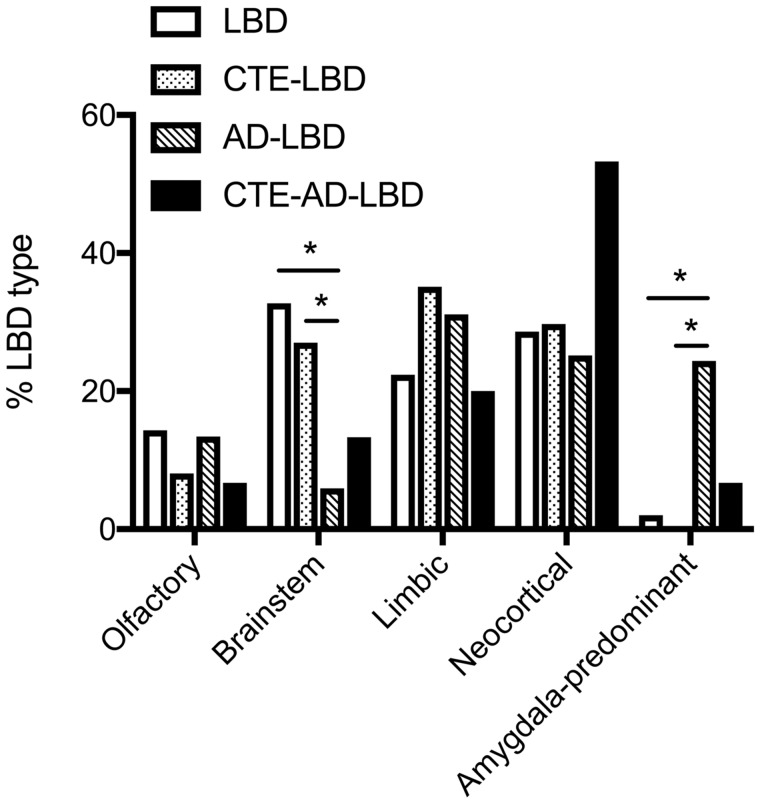
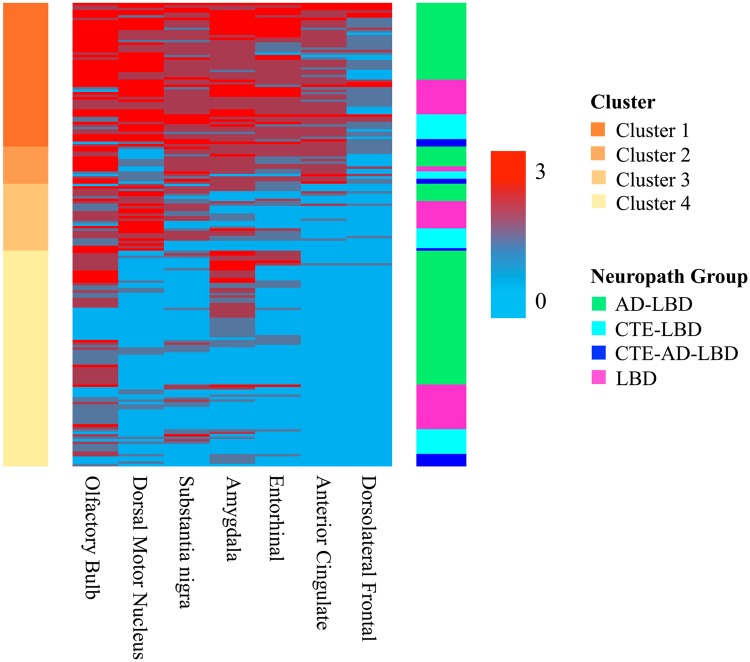
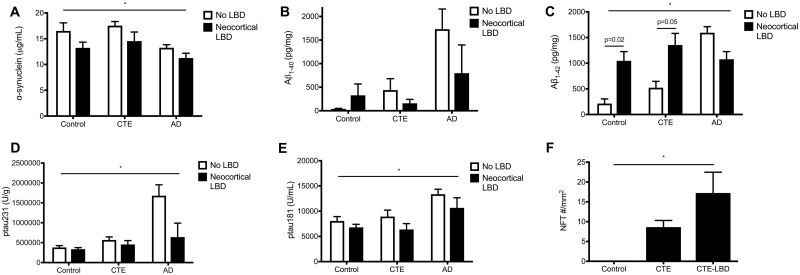
Traumatic brain injury has been associated with increased risk of Parkinson disease and parkinsonism, and parkinsonism and Lewy body disease (LBD) can occur with chronic traumatic encephalopathy (CTE). To test whether contact sports and CTE are associated with LBD, we compared deceased contact sports athletes (n = 269) to cohorts from the community (n = 164) and the Boston University Alzheimer disease (AD) Center (n = 261). Participants with CTE and LBD were more likely to have β-amyloid deposition, dementia, and parkinsonism than CTE alone (p < 0.05). Traditional and hierarchical clustering showed a similar pattern of LBD distribution in CTE compared to LBD alone that was most frequently neocortical, limbic, or brainstem. In the community-based cohort, years of contact sports play were associated with neocortical LBD (OR = 1.30 per year, p = 0.012), and in a pooled analysis a threshold of >8 years of play best predicted neocortical LBD (ROC analysis, OR = 6.24, 95% CI = 1.5-25, p = 0.011), adjusting for age, sex, and APOE ɛ4 allele status. Clinically, dementia was significantly associated with neocortical LBD, CTE stage, and AD; parkinsonism was associated with LBD pathology but not CTE stage. Contact sports participation may increase risk of developing neocortical LBD, and increased LBD frequency may partially explain extrapyramidal motor symptoms sometimes observed in CTE.
Figures
References
-
- Guerriero RM, Proctor MR, Mannix R, et al. Epidemiology, trends, assessment and management of sport-related concussion in United States high schools. Curr Opin Pediatr 2012;24:696–701 - PubMed
-
- Singh R, Meier TB, Kuplicki R, et al. Relationship of collegiate football experience and concussion with hippocampal volume and cognitive outcomes. JAMA 2014;311:1883–8 - PubMed
-
- Poole VN, Abbas K, Shenk TE, et al. MR spectroscopic evidence of brain injury in the non-diagnosed collision sport athlete. Dev Neuropsychol 2014;39:459–73 - PubMed
-
- Nauman EA, Breedlove KM, Breedlove EL, et al. Post-season neurophysiological deficits assessed by ImPACT and fMRI in athletes competing in American football. Dev Neuropsychol 2015;40:85–91 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- RF1 AG057768/AG/NIA NIH HHS/United States
- R01 NS017950/NS/NINDS NIH HHS/United States
- R01 AG016495/AG/NIA NIH HHS/United States
- U01 NS086659/NS/NINDS NIH HHS/United States
- K23 NS102399/NS/NINDS NIH HHS/United States
- R01 AG008122/AG/NIA NIH HHS/United States
- N01 HC025195/HL/NHLBI NIH HHS/United States
- I01 CX001038/CX/CSRD VA/United States
- I01 BX003527/BX/BLRD VA/United States
- F32 NS096803/NS/NINDS NIH HHS/United States
- R56 AG057768/AG/NIA NIH HHS/United States
- RF1 AG054156/AG/NIA NIH HHS/United States
- P30 AG013846/AG/NIA NIH HHS/United States
- I01 BX002466/BX/BLRD VA/United States
- K23 AG046377/AG/NIA NIH HHS/United States
- R01 AG033040/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
