

Unusual case of chronic recurrent multifocal osteomyelitis
- PMID: 30053822
- PMCID: PMC6062932
- DOI: 10.1186/s12969-018-0267-4
Unusual case of chronic recurrent multifocal osteomyelitis
Abstract
Background: Chronic recurrent multifocal osteomyelitis (CRMO) is a rare auto-inflammatory bone disorder that primarily affects young girls, with a mean age of 10 years at onset. Generally, it is a self-limited disease. However, recent data indicate that more than 50% of patients have a chronic persistent disease and about 20% a recurring course of this condition. Also, there are more cases reported with associated auto-inflammatory and autoimmune diseases. In this case report, we present a rare case of sporadic CRMO in which the patient eventually developed C-ANCA (cytoplasmic anti-neutrophil cytoplasmic antibodies)-associated renal vasculitis and hyperparathyroidism.
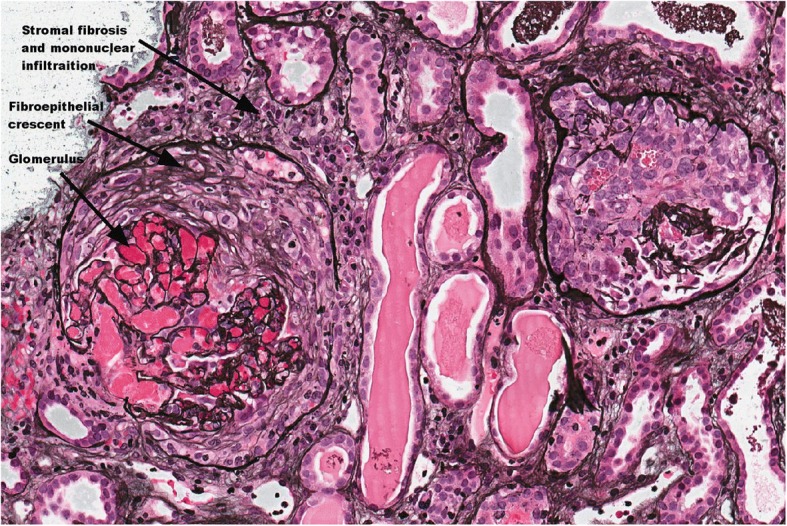
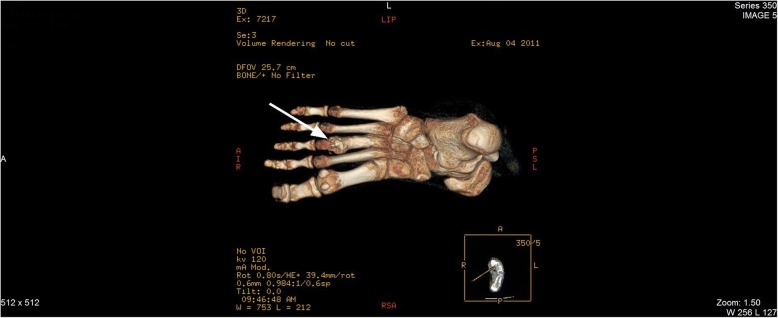
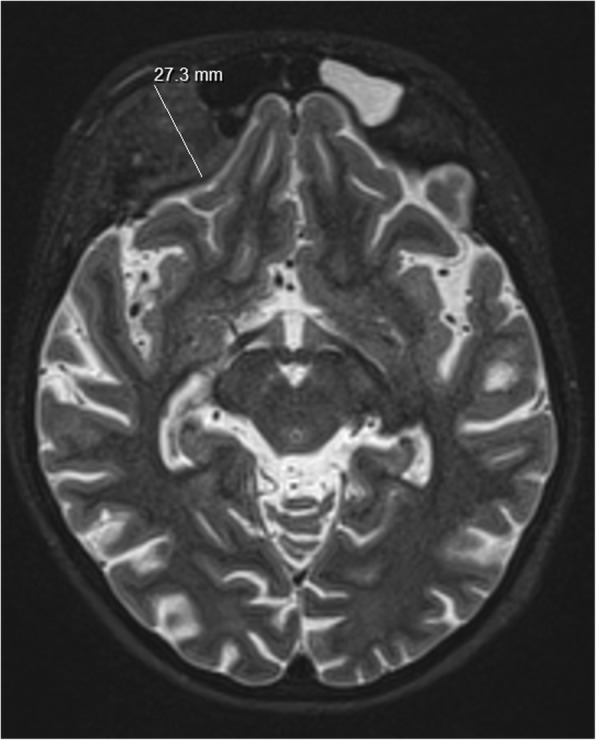
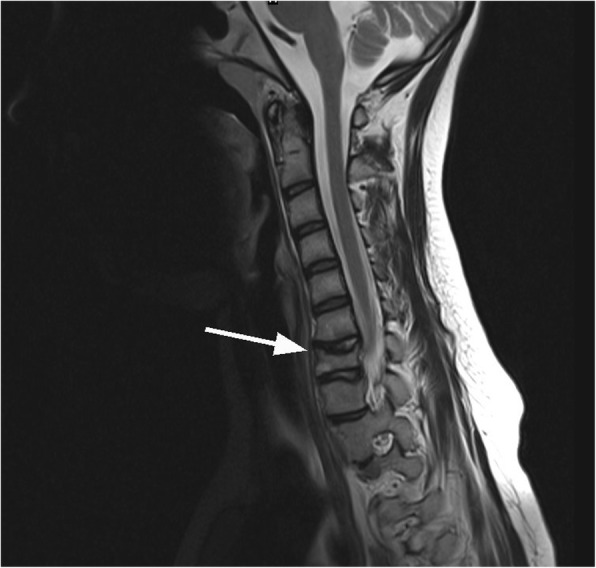
Case presentation: A 14 year old female patient was brought to the emergency department with a sudden onset of left leg pain and oedema. After physical evaluation and initial investigation, she was diagnosed with femoral and pelvic deep vein thrombosis. While searching for possible thrombosis causes, osteomyelitis of the left leg was identified. Additional CT and MRI scans hinted at the CRMO diagnosis. Due to the multifocal lesions of CRMO, endocrinological evaluation of calcium metabolism was done. The results showed signs of hyperparathyroidism with severe hypocalcaemia. Moreover, when kidney damage occurred and progressed, a kidney biopsy was performed, revealing a C-ANCA associated renal vasculitis. Treatment was started with cyclophosphamide and prednisolone according to the renal vasculitis management protocol. Severe metabolic disturbances and hyperparathyroidism were treated with alfacalcidol, calcium and magnesium supplements. Secondary glomerulonephritis (GN) associated hypertension was treated with ACE (angiotenzine converting enzyme) inhibitors. Anticoagulants were prescribed for deep vein thrombosis. After 1.5 years of treatment, the patient is free of complaints. All microelement and parathormone levels are within normal range. Kidney function is now normal. To date, there are no clinical or diagnostic signs of deep vein thrombosis.
Conclusions: This case report presents a complex immunodysregulatory disorder with both auto-inflammatory and autoimmune processes. We hypothesize that the long lasting active inflammation of CRMO may induce an autoimmune response and result in concomitant diseases like C-ANCA-associated vasculitis in our patient. Any potential specific pathogenic relationships between these two rare pathologies may need to be further studied. Furthermore, there is a lack of specific biomarkers for CRMO and more studies are necessary to identify CRMO's characteristic patterns and how to best monitor disease progression.
Keywords: Auto-inflammation; Autoimmune; C-ANCA; CRMO; GPA; Hyperparathyroidism; Paediatric; Renal vasculitis.
Conflict of interest statement
Authors’ information
AS is a paediatric rheumatology resident at The Lithuanian University of Health Sciences (LUHS) and the Hospital of Lithuanian University of Health Sciences Kauno Klinikos (HLUHS KK).
RS is an Associated Professor at the Paediatric Clinic of LUHS, and is Head of the Department of Paediatric Rheumatology and Cardiology at the HLUHS KK.
JK is a paediatric heamatology doctor at the Department of Paediatric Oncology at the HLUHS KK.
EJ is a lecturer at the Endocrinology Clinic of the LUHS and Head of the Department of Paediatric Endocrinology at the HLUHS KK.
RU is a lecturer at the Radiology Clinic of the LUHS and a radiologist in the Radiology Department at the HLUHS KK.
LJ is a lecturer at the Paediatric Clinic of the LUHS, post-doc at the Department of Physiology and Pharmacology of the LUHS, and a paediatric pulmonology doctor in the Paediatric department at the HLUHS KK.
Ethics approval and consent to participate
The consent to use anonymic patient data for the case report was obtained from the parent of the patient.
Consent for publication
Written informed consent for publication of their clinical details and clinical images was obtained from the parent of the patient. A copy of the consent form is available for review by the Editor of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- PRINTO. Eurofever registry. PRINTO web site. PRINTO. [Cited: June 12, 2017.] https://www.printo.it/eurofever/eurofever_registry.asp.
-
- Orphanet. Orphanet Rare Disease Web site. [Cited: June 12, 2017] http://www.orpha.net.
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
