

A robot-based gait training therapy for pediatric population with cerebral palsy: goal setting, proposal and preliminary clinical implementation
- PMID: 30053857
- PMCID: PMC6063005
- DOI: 10.1186/s12984-018-0412-9
A robot-based gait training therapy for pediatric population with cerebral palsy: goal setting, proposal and preliminary clinical implementation
Abstract
Background: The use of robotic trainers has increased with the aim of improving gait function in patients with limitations. Nevertheless, there is an absence of studies that deeply describe detailed guidelines of how to correctly implement robot-based treatments for gait rehabilitation. This contribution proposes an accurate robot-based training program for gait rehabilitation of pediatric population with Cerebral Palsy (CP).
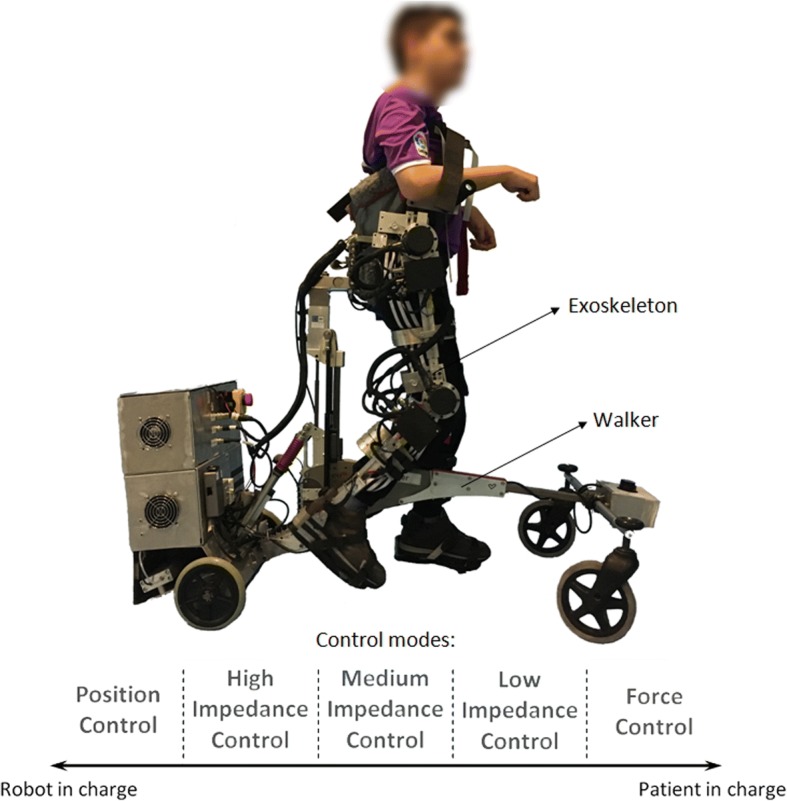
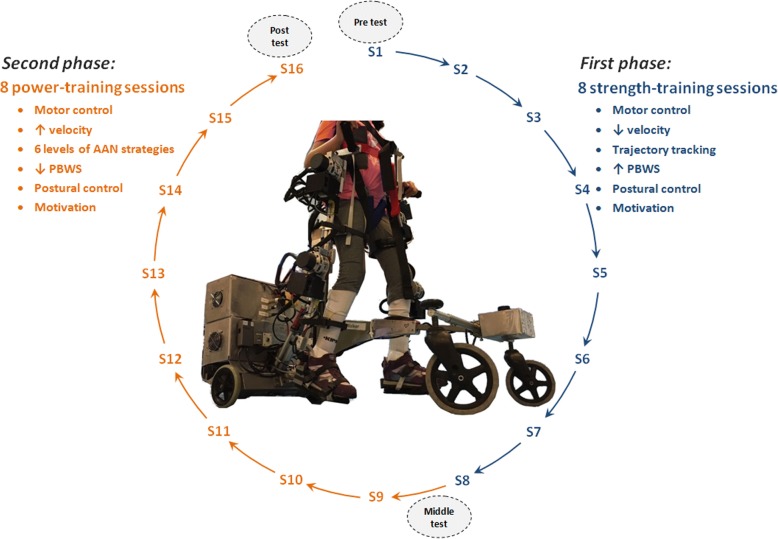
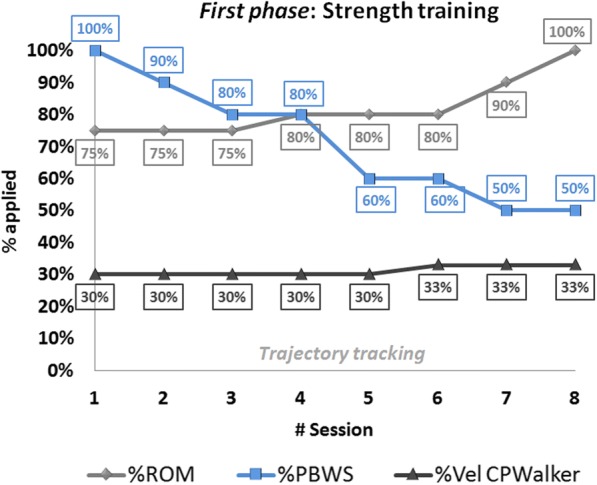
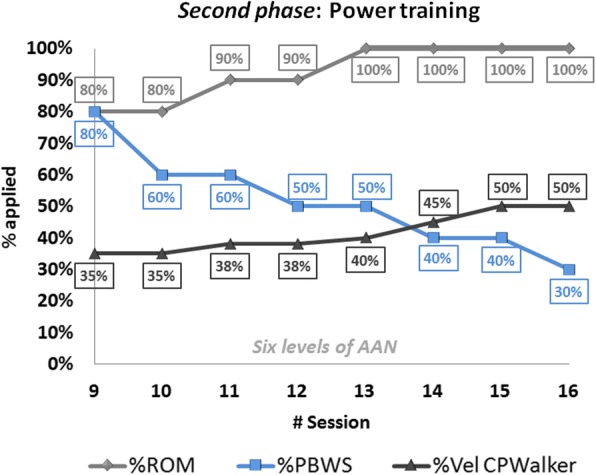
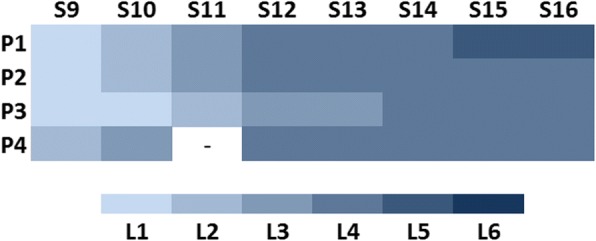
Methods: The program is focused on the achievement of some specifications defined by the International Classification of Functioning, Disability and Health framework, Children and Youth version (ICF-CY). It is framed on 16 non-consecutive sessions where motor control, strength and power exercises of lower limbs are performed in parallel with a postural control strategy. A clinical evaluation with four pediatric patients with CP using the CPWalker robotic platform is presented.
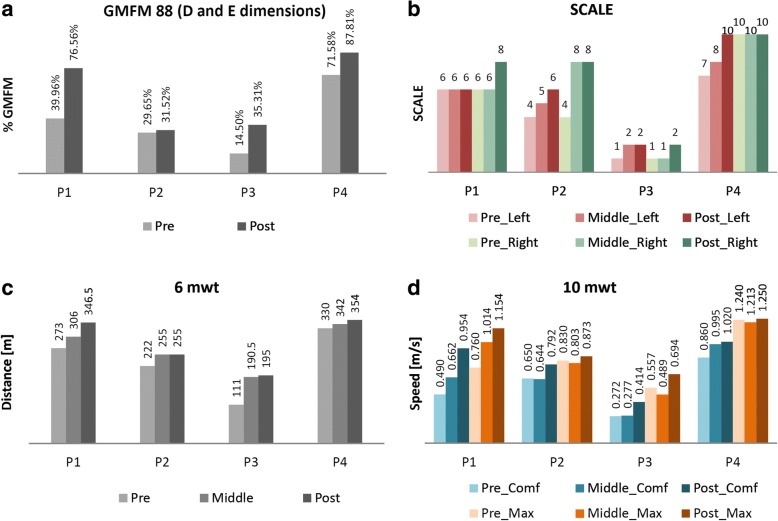
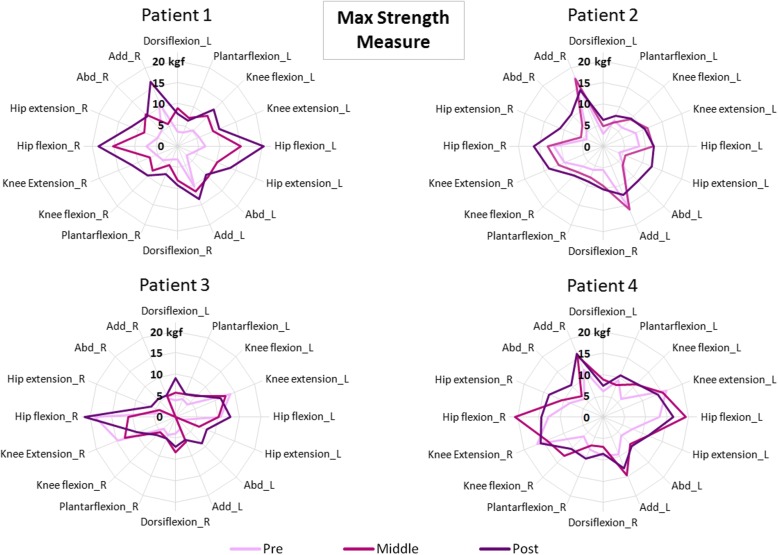
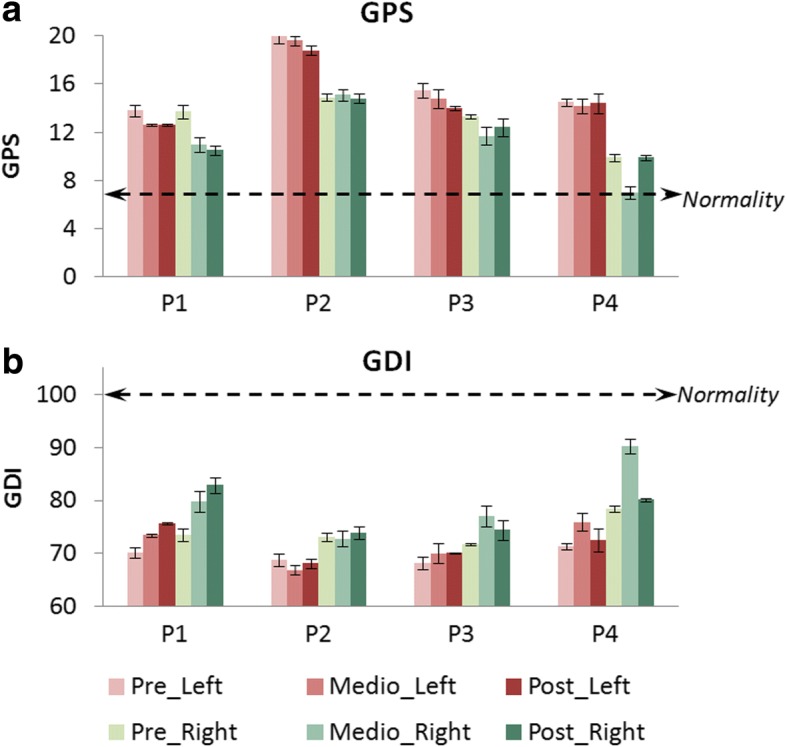
Results: The preliminary evaluation with patients with CP shows improvements in several aspects as strength (74.03 ± 40.20%), mean velocity (21.46 ± 33.79%), step length (17.95 ± 20.45%) or gait performance (e.g. 66 ± 63.54% in Gross Motor Function Measure-88 items, E and D dimensions).
Conclusions: The improvements achieved in the short term show the importance of working strength and power functions meanwhile over-ground training with postural control. This research could serve as preliminary support for future clinical implementations in any robotic device.
Trial registration: The study was carried out with the number R-0032/12 from Local Ethical Committee of the Hospital Infantil Niño Jesús. Public trial registered on March 23, 2017: ISRCTN18254257 .
Keywords: Cerebral palsy; Exoskeleton; Gait; Rehabilitation; Robotic training; Therapy.
Conflict of interest statement
Ethics approval and consent to participate
The Local Ethical Committee of the “Hospital Infantil Universitario Niño Jesús” gave approval to the study and warranted its accordance with the Declaration of Helsinki. The study was carried out with the number R-0032/12 from Local Ethical Committee of the Hospital, and was publicly registered with the number ISRCTN18254257 as clinical trial. All patients and families were informed beforehand and provided consent through parents to participate.
Consent for publication
Consent for publication has been given by parents or legal guardians of involved patients.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Palisano R, Rosenbaum P, Walter S, Russell D, Wood E, Galuppi B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol. 1997;39:214–23. PMID: 9183258. - PubMed
-
- Dietz V. Clinical aspects for the application of robotics in locomotor neurorehabilitation. In: Reinkensmeyer DJ, Dietz V, editors. Neurorehabilitation Technol: Springer; 2016. p. 209–21. 10.1007/978-3-319-28603-7_11.
-
- Bayón C, Raya R, Lara SL, Ramírez Ó, Serrano J, Rocon E. Robotic therapies for children with cerebral palsy: a systematic review. Transl Biomed. 2016;7:1–10. doi: 10.21767/2172-0479.100044. - DOI
-
- Diaz I, Gil J, Sanchez E. Lower-limb robotic rehabilitation: literature review and challenges, J robot. 2011.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
