

Prevalence and Costs of Discharge Diagnoses in Inpatient General Internal Medicine: a Multi-center Cross-sectional Study
- PMID: 30054888
- PMCID: PMC6206337
- DOI: 10.1007/s11606-018-4591-7
Prevalence and Costs of Discharge Diagnoses in Inpatient General Internal Medicine: a Multi-center Cross-sectional Study
Abstract
Background: Understanding the most common and costly conditions treated by inpatient general medical services is important for implementing quality improvement, developing health policy, conducting research, and designing medical education.
Objective: To determine the prevalence and cost of conditions treated on general internal medicine (GIM) inpatient services.
Design: Retrospective cross-sectional study involving 7 hospital sites in Toronto, Canada.
Participants: All patients discharged between April 1, 2010 and March 31, 2015 who were admitted to or discharged from an inpatient GIM service.
Main measures: Hospital administrative data were used to identify diagnoses and costs associated with admissions. The primary discharge diagnosis was identified for each admission and categorized into clinically relevant and mutually exclusive categories using the Clinical Classifications Software (CCS) tool.
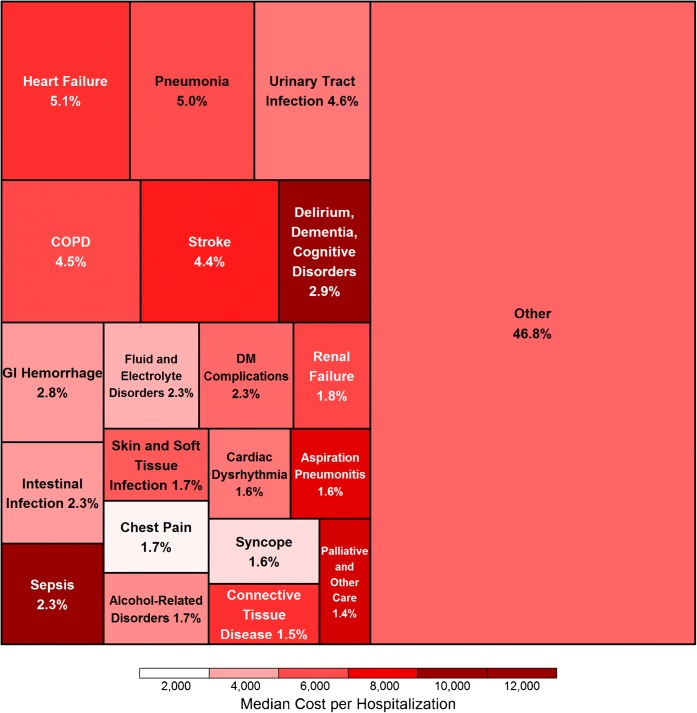
Key results: Among 148,442 admissions, the most common primary discharge diagnoses were heart failure (5.1%), pneumonia (5.0%), urinary tract infection (4.6%), chronic obstructive pulmonary disease (4.5%), and stroke (4.4%). The prevalence of the 20 most common conditions was significantly correlated across hospitals (correlation coefficients ranging from 0.55 to 0.95, p ≤ 0.01 for all comparisons). No single condition represented more than 5.1% of all admissions or more than 7.9% of admissions at any hospital site. The costliest conditions were stroke (median cost $7122, interquartile range 5587-12,354, total cost $94,199,422, representing 6.0% of all costs) and the group of delirium, dementia, and cognitive disorders (median cost $12,831, IQR 9539-17,509, total cost $77,372,541, representing 4.9% of all costs). The 10 most common conditions accounted for only 36.2% of hospitalizations and 36.8% of total costs. The remaining hospitalizations included 223 different CCS conditions.
Conclusions: GIM services care for a markedly heterogeneous population but the most common conditions were similar across 7 hospitals. The diversity of conditions cared for in GIM may be challenging for healthcare delivery and quality improvement. Initiatives that cut across individual diseases to address processes of care, patient experience, and functional outcomes may be more relevant to a greater proportion of the GIM population than disease-specific efforts.
Keywords: cost; diagnoses; health services research; hospitalist; internal medicine.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
Comment in
-
Capsule Commentary on Verma et al., Prevalence and Costs of Discharge Diagnoses in Inpatient General Internal Medicine: a Multi-center Cross-sectional Study.J Gen Intern Med. 2018 Nov;33(11):1956. doi: 10.1007/s11606-018-4641-1. J Gen Intern Med. 2018. PMID: 30206791 Free PMC article. No abstract available.
References
-
- Verma A, Bhatia S. A policy framework for health systems to promote triple aim innovation. Healthc Pap. 2016;15(3):9–23. - PubMed
-
- Soong C, Fan E, Howell EE, et al. Characteristics of hospitalists and hospitalist programs in the united states and canada. J Clin Outcomes Manag. 2009;16(2):69–74.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
