

Impact of radiologically stratified exacerbations: insights into pneumonia aetiology in COPD
- PMID: 30055608
- PMCID: PMC6064093
- DOI: 10.1186/s12931-018-0842-8
Impact of radiologically stratified exacerbations: insights into pneumonia aetiology in COPD
Abstract
Background: COPD patients have increased risk of developing pneumonia, which is associated with poor outcomes. It can be symptomatically indistinguishable from exacerbations, making diagnosis challenging. Studies of pneumonia in COPD have focused on hospitalised patients and are not representative of the ambulant COPD population. Therefore, we sought to determine the incidence and aetiology of acute exacerbation events with evidence of pneumonic radiographic infiltrates in an outpatient COPD cohort.
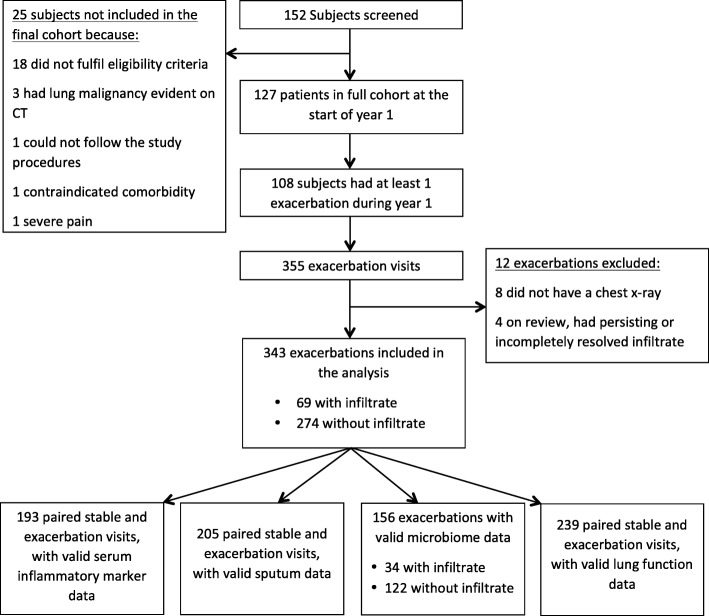
Methods: One hundred twenty-seven patients with moderate to very severe COPD aged 42-85 years underwent blood and sputum sampling over one year, at monthly stable visits and within 72 h of exacerbation symptom onset. 343 exacerbations with chest radiographs were included.
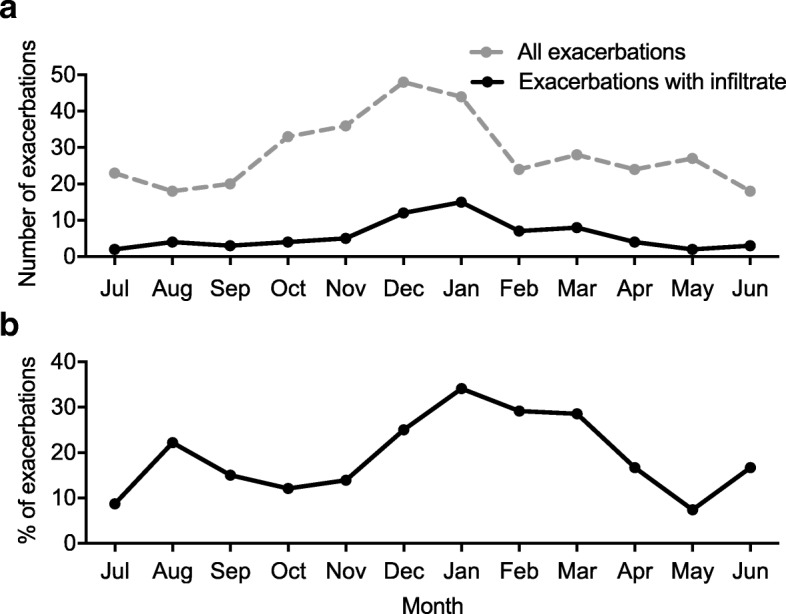
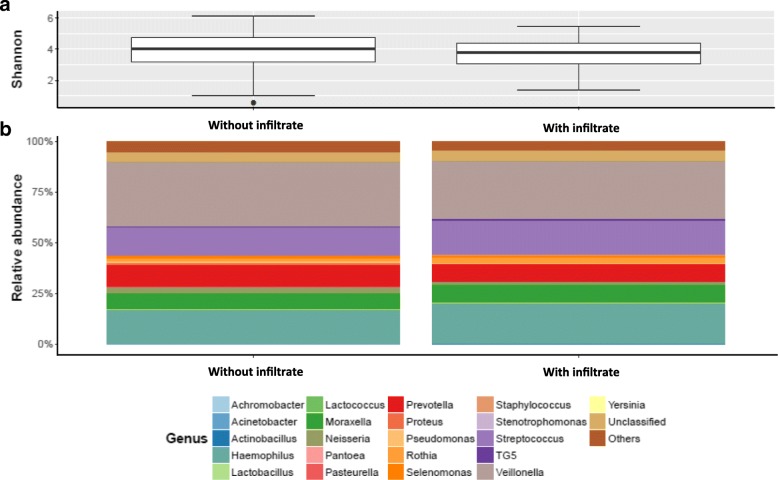
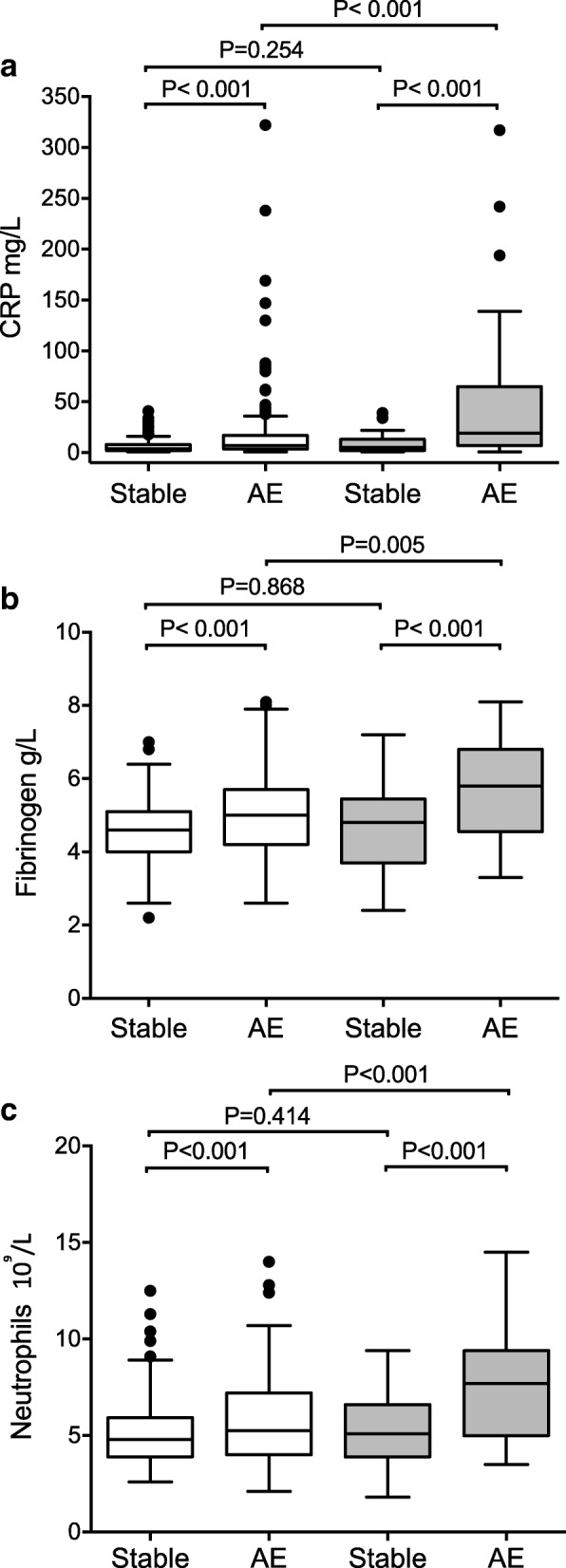
Results: 20.1% of exacerbations had pneumonic infiltrates. Presence of infiltrate was highly seasonal (Winter vs summer OR 3.056, p = 0.027). In paired analyses these exacerbation events had greater increases in systemic inflammation. Bacterial detection rate was higher in the pneumonic group, with Haemophilus influenzae the most common bacteria in both radiological groups. Viral detection and sputum microbiota did not differ with chest radiograph appearance.
Conclusions: In an outpatient COPD cohort, pneumonic infiltrates at exacerbation were common, and associated with more intense inflammation. Bacterial pathogen detection and lung microbiota were not distinct, suggesting that exacerbations and pneumonia in COPD share common infectious triggers and represent a continuum of severity rather than distinct aetiological events.
Trial registration: Trial registration Number: NCT01360398 .
Keywords: COPD; Exacerbations; Infiltrates; Pneumonia.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Southampton and South West Hampshire Research Ethics Committee. All participants provided written informed consent.
Consent for publication
Not applicable.
Competing interests
TMAW has received reimbursement for travel and meeting attendance from Boehringer Ingelheim and AstraZeneca, outside of the submitted work. SB received grants and assistance in travel to conferences from GSK outside of the submitted work. SCC received a grant from Pfizer outside of the submitted work. KJS received grants from Asthma UK (08/026) and BMA HC Roscoe Award outside of the submitted work, and he has a patent PCT/GB2010/050821 “Ex Vivo Modelling of Therapeutic Interventions” pending. EA, JMD and CL are employees of the GSK group of companies. EA and JMD hold shares/restricted shares in the GSK group of companies. KJS, VK, NPW, KO, SW, and TMAW received an institutional grant from the GSK group of companies to conduct this study. AW, NAC, SH and AT declare no conflict of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Miravitlles M, Ferrer M, Pont A, Zalacain R, Alvarez-Sala JL, Masa F, Verea H, Murio C, Ros F, Vidal R. Effect of exacerbations on quality of life in patients with chronic obstructive pulmonary disease: a 2 year follow up study. Thorax. 2004;59:387–395. doi: 10.1136/thx.2003.008730. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
