

Distinguishing Highly Asymmetric Keratoconus Eyes Using Combined Scheimpflug and Spectral-Domain OCT Analysis
- PMID: 30055838
- PMCID: PMC6246819
- DOI: 10.1016/j.ophtha.2018.06.020
Distinguishing Highly Asymmetric Keratoconus Eyes Using Combined Scheimpflug and Spectral-Domain OCT Analysis
Abstract
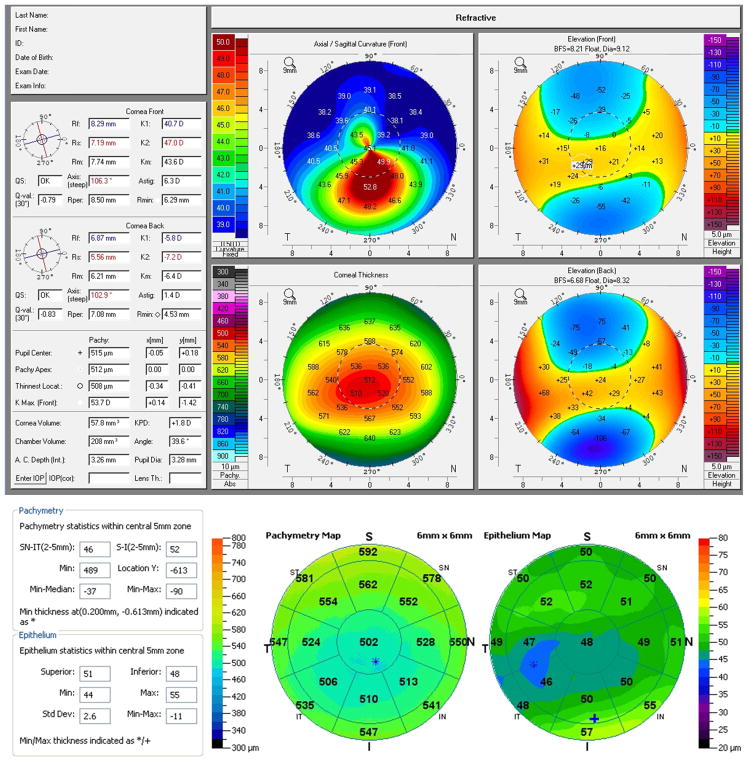
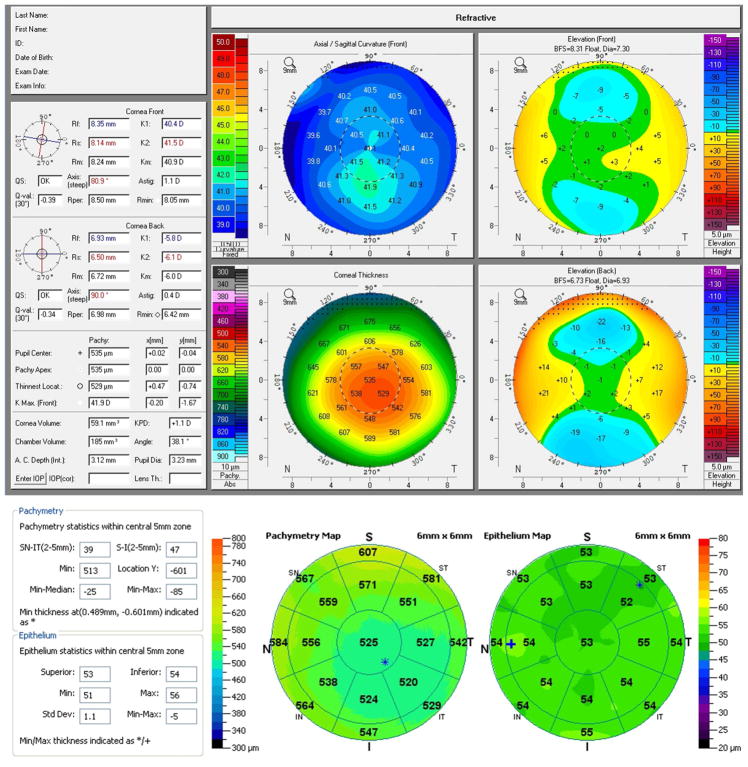
Purpose: To determine optimal objective, machine-derived variables and variable combinations from Scheimpflug and spectral-domain (SD) OCT imaging to distinguish the clinically unaffected eye in patients with asymmetric keratoconus (AKC) from a normal control population.
Design: Retrospective case-control study.
Participants: Thirty clinically unaffected eyes with no physical findings on slit-lamp examination, no definitive abnormalities on corneal imaging, and corrected distance acuity of 20/20 or better from 30 patients with highly AKC eyes and 60 eyes from 60 normal control patients who had undergone uneventful LASIK with at least 2 years of stable follow-up (controls).
Methods: Scheimpflug and SD OCT imaging were obtained in all eyes, and receiver operating characteristic (ROC) curves were generated to determine area under the curve (AUC), sensitivity, and specificity for each machine-derived variable and variable combination.
Main outcome measures: Distinguishing AKC eyes from controls as determined by AUC, sensitivity, and specificity.
Results: No individual machine-derived metric from Scheimpflug or SD OCT technology yielded an AUC higher than 0.75. Combining 5 Scheimpflug metrics (index height decentration [IHD], index vertical asymmetry [IVA], pachymetry apex, inferior-superior value, and Ambrosio's Relational Thickness Maximum [ARTmax]) yielded the best Scheimpflug results (AUC 0.86, sensitivity 83%, specificity 83%). Combining 11 SD OCT thickness metrics (minimum-median, temporal outer, superior nasal outer, minimum, epithelium minimum-maximum, epithelial standard deviation, superior inner, superior outer, superior temporal outer, superior nasal inner, central) yielded the best SD OCT results (AUC 0.96, sensitivity 89%, specificity 89%). Combining 13 total Scheimpflug/SD OCT metrics yielded the best results overall (AUC 1.0, sensitivity 100%, specificity 100%). The most impactful variables in combined models included epithelial thickness variability and total focal corneal thickness variability from SD OCT and anterior curvature and topometric indices from Scheimpflug technology. No posterior corneal metrics were impactful in modeling.
Conclusions: Individual machine-derived metrics from Scheimpflug and SD OCT imaging poorly distinguished normal eyes from minimally affected eyes from patients with highly AKC. Combined SD OCT metrics performed better than combined Scheimpflug metrics. Combining anterior curvature and asymmetry indices from Scheimpflug with regional total thickness and epithelial thickness variability metrics from SD OCT clearly distinguished the 2 populations. Posterior corneal indices were not useful in distinguishing populations.
Copyright © 2018 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest/Financial Disclosures Statement
Figures


Comment in
-
The Future of Keratoconus Screening with Artificial Intelligence.Ophthalmology. 2018 Dec;125(12):1872-1873. doi: 10.1016/j.ophtha.2018.08.019. Ophthalmology. 2018. PMID: 30454713 No abstract available.
-
Re: Hwang et al.: Distinguishing highly asymmetric keratoconus eyes using combined Scheimpflug and spectral-domain OCT analysis (Ophthalmology. 2018;125:1862-1871).Ophthalmology. 2019 Apr;126(4):e26. doi: 10.1016/j.ophtha.2018.10.034. Ophthalmology. 2019. PMID: 30910043 No abstract available.
-
Reply.Ophthalmology. 2019 Apr;126(4):e27-e28. doi: 10.1016/j.ophtha.2018.10.035. Ophthalmology. 2019. PMID: 30910044 No abstract available.
-
Re: Hwang et al.: Distinguishing highly asymmetric keratoconus eyes using combined Scheimpflug and spectral-domain OCT analysis (Ophthalmology. 2018;125:1862-1871).Ophthalmology. 2019 Jul;126(7):e55-e56. doi: 10.1016/j.ophtha.2019.02.014. Ophthalmology. 2019. PMID: 31229016 No abstract available.
-
Reply.Ophthalmology. 2019 Jul;126(7):e56-e57. doi: 10.1016/j.ophtha.2019.02.013. Ophthalmology. 2019. PMID: 31229017 No abstract available.
-
Re: Hwang et al.: Distinguishing highly asymmetric keratoconus eyes using combined Scheimpflug and spectral-domain OCT analysis (Ophthalmology. 2018;125:1862-1871).Ophthalmology. 2019 Jul;126(7):e57-e58. doi: 10.1016/j.ophtha.2019.02.008. Ophthalmology. 2019. PMID: 31229018 No abstract available.
-
Reply.Ophthalmology. 2019 Jul;126(7):e58. doi: 10.1016/j.ophtha.2019.02.012. Ophthalmology. 2019. PMID: 31229019 No abstract available.
References
-
- Rabinowitz YS, McDonnell PJ. Computer-assisted corneal topography in keratoconus. Refract Corneal Surg. 1989;5(6):400–408. - PubMed
-
- Klyce SD, Karon MD, Smolek MK. Screening patients with the corneal navigator. J Refract Surg. 2005;21(5 Suppl):S617–622. - PubMed
-
- Randleman JB, Russell B, Ward MA, Thompson KP, Stulting RD. Risk factors and prognosis for corneal ectasia after LASIK. Ophthalmology. 2003;110(2):267–275. - PubMed
-
- Binder PS, Lindstrom RL, Stulting RD, et al. Keratoconus and corneal ectasia after LASIK. J Cataract Refract Surg. 2005;31(11):2035–2038. - PubMed
-
- Randleman JB, Woodward M, Lynn MJ, Stulting RD. Risk assessment for ectasia after corneal refractive surgery. Ophthalmology. 2008;115(1):37–50. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
