

Primary Care Provider Practice Patterns and Barriers to Hepatocellular Carcinoma Surveillance
- PMID: 30056183
- PMCID: PMC7212522
- DOI: 10.1016/j.cgh.2018.07.029
Primary Care Provider Practice Patterns and Barriers to Hepatocellular Carcinoma Surveillance
Abstract
Background & aims: Low rates of hepatocellular carcinoma (HCC) surveillance are primarily due to provider-related process failures. However, few studies have evaluated primary care provider (PCP) practice patterns, attitudes, and barriers to HCC surveillance at academic tertiary care referral centers.
Methods: We conducted a web-based survey of PCPs at 2 tertiary care referral centers (133 providers) from June 2017 through December 2017. The survey was adapted from pretested surveys and included questions about practice patterns, attitudes, and barriers to HCC surveillance. We used the Fisher exact and Mann-Whitney rank-sum tests to identify factors associated with adherence to HCC surveillance recommendations, for categoric and continuous variables, respectively.
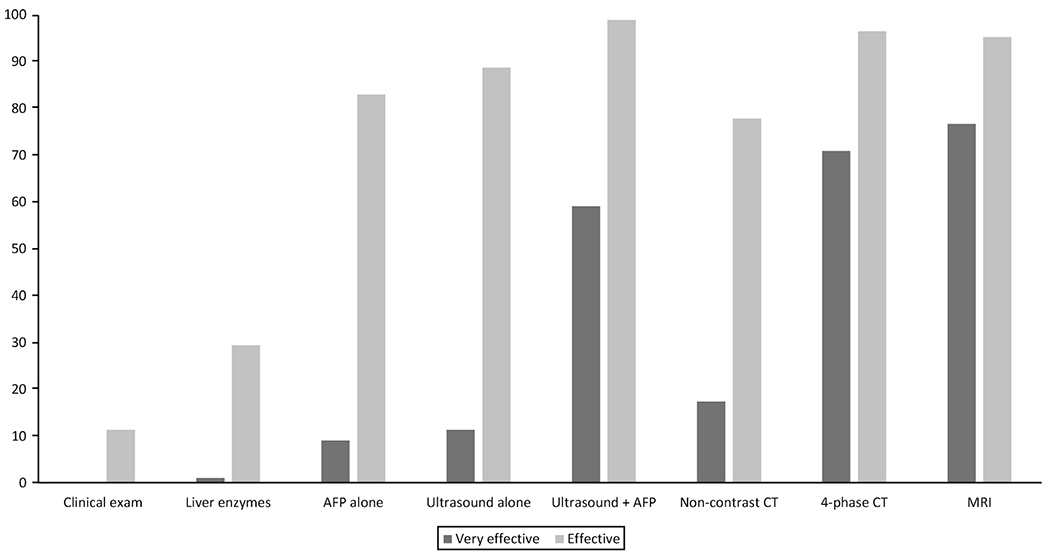
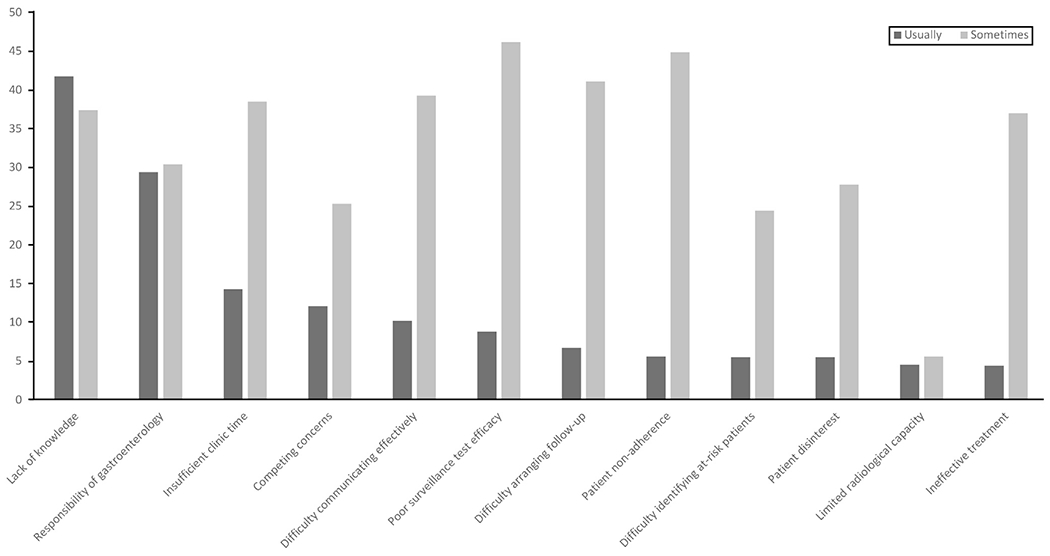
Results: We obtained a provider-level response rate of 75% and clinic-level response rate of 100% (133 providers). Whereas most PCPs performed HCC surveillance themselves, one-third deferred surveillance to subspecialists and referred patients to a hepatology clinic. Providers believed the combination of ultrasound and α-fetoprotein analysis to be highly effective for early stage tumor detection and reported using the combination for assessment of most patients. However, PCPs were more likely to use computed tomography- or magnetic resonance imaging-based surveillance for patients with nonalcoholic steatohepatitis or decompensated cirrhosis. Most providers believed HCC surveillance to be efficacious for early tumor detection and increasing survival. However, they desired increased high-quality evidence to characterize screening benefits and harms. Providers expressed notable misconceptions about HCC surveillance, including the role for measurement of liver enzyme levels in HCC surveillance and cost effectiveness of surveillance in patients without cirrhosis. They also reported barriers, including not being up to date on HCC surveillance recommendations, limited time in the clinic, and competing clinical concerns.
Conclusions: In a web-based survey, PCPs reported misconceptions and barriers to HCC surveillance. This indicates the need for interventions, including provider education, to improve HCC surveillance effectiveness in clinical practice.
Keywords: Early Detection; Liver Cancer; NASH; Screening; Survey.
Copyright © 2019 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest
The authors disclose no conflicts.
Figures
References
-
- European Association for the Study of the Liver, European Organisation for Research and Treatment of Cancer. EASLEORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol 2012;56:908–943. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin 2018;68:7–30. - PubMed
-
- El-Serag HB. Hepatocellular carcinoma. N Engl J Med 2011; 365:1118–1127. - PubMed
-
- Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet 2018;391:1301–1314. - PubMed
-
- Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018; 67:358–380. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
