

Right ventricular mechanics and contractility after aortic valve replacement surgery: a randomised study comparing minimally invasive versus conventional approach
- PMID: 30057770
- PMCID: PMC6059303
- DOI: 10.1136/openhrt-2018-000842
Right ventricular mechanics and contractility after aortic valve replacement surgery: a randomised study comparing minimally invasive versus conventional approach
Abstract
Objective: Minimally invasive aortic valve replacementsurgery (MIAVR) is an alternative surgical technique to conventional aortic valve replacement surgery (AVR) in selected patients. The randomised study Cardiac Function after Minimally Invasive Aortic Valve Implantation (CMILE) showed that right ventricular (RV) longitudinal function was reduced after both MIAVR and AVR, but the reduction was more pronounced following AVR. However, postoperative global RV function was equally impaired in both groups. The purpose of this study was to explore alterations in RV mechanics and contractility following MIAVR as compared with AVR.
Methods: A predefined post hoc analysis of CMILE consisting of 40 patients with severe aortic valve stenosis who were eligible for isolated surgical aortic valve replacement were randomised to MIAVR or AVR. RV function was assessed by echocardiography prior to surgery and 40 days post-surgery.
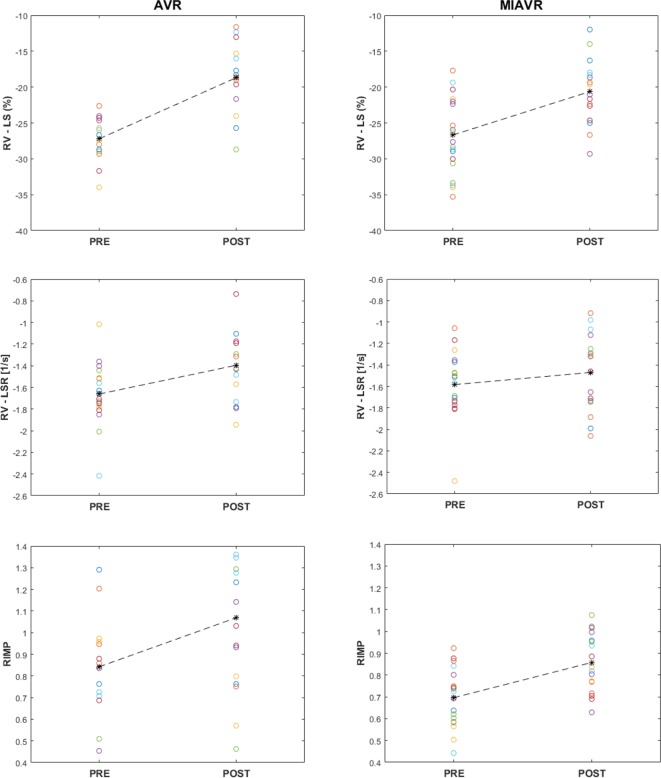
Results: Comparing preoperative to postoperative values, RV longitudinal strain rate was preserved following MIAVR (-1.5±0.5 vs -1.5±0.4 1/s, p=0.84) but declined following AVR (-1.7±0.3 vs -1.4±0.3 1/s, p<0.01). RV longitudinal strain reduced following AVR (-27.4±2.9% vs -18.8%±4.7%, p<0.001) and MIAVR (-26.5±5.3% vs -20.7%±4.5%, p<0.01). Peak systolic velocity of the lateral tricuspid annulus reduced by 36.6% in the AVR group (9.3±2.1 vs 5.9±1.5 cm/s, p<0.01) and 18.8% in the MIAVR group (10.1±2.9 vs 8.2±1.4 cm/s, p<0.01) when comparing preoperative values with postoperative values.
Conclusions: RV contractility was preserved following MIAVR but was deteriorated following AVR. RV longitudinal function reduced substantially following AVR. A decline in RV longitudinal function was also observed following MIAVR, however, to a much lesser extent.
Keywords: aortic valve disease; cardiac function; echocardiography; minimally invasive; surgery-valve.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Unsworth B, Casula RP, Yadav H, et al. Contrasting effect of different cardiothoracic operations on echocardiographic right ventricular long axis velocities, and implications for interpretation of post-operative values. Int J Cardiol 2013;165:151–60. 10.1016/j.ijcard.2011.08.031 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources