

Chronic pulmonary embolism: diagnosis
- PMID: 30057874
- PMCID: PMC6039808
- DOI: 10.21037/cdt.2018.01.09
Chronic pulmonary embolism: diagnosis
Abstract
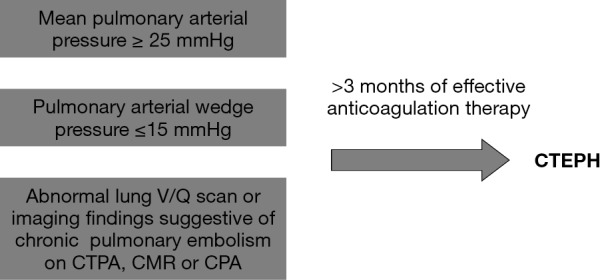
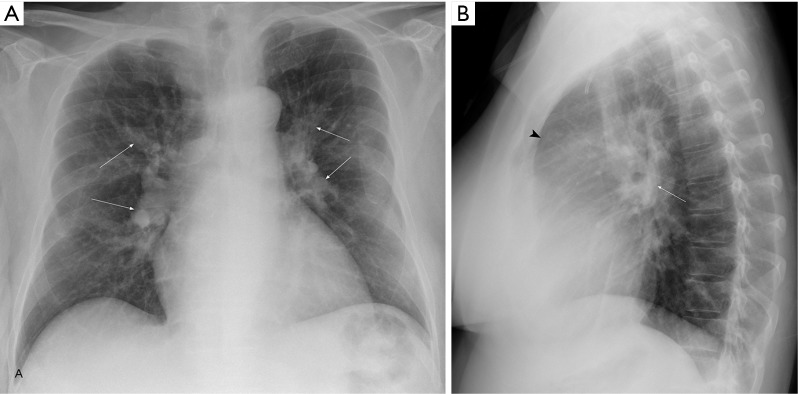
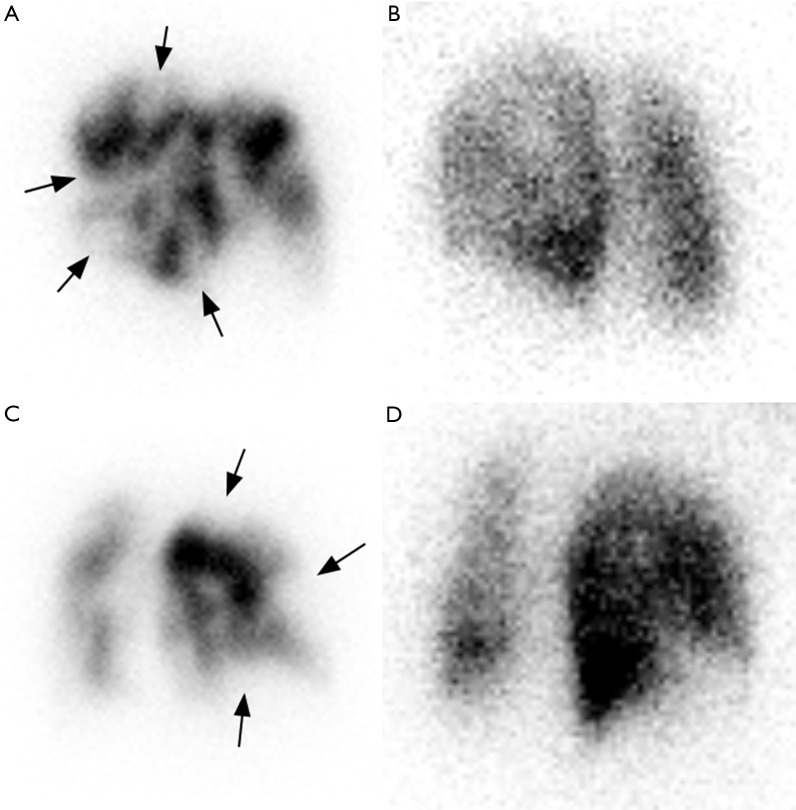
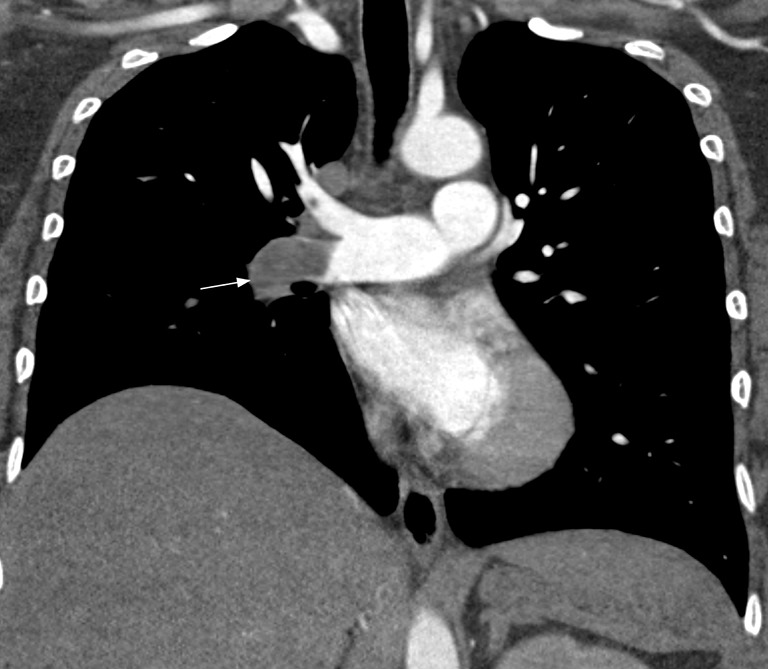
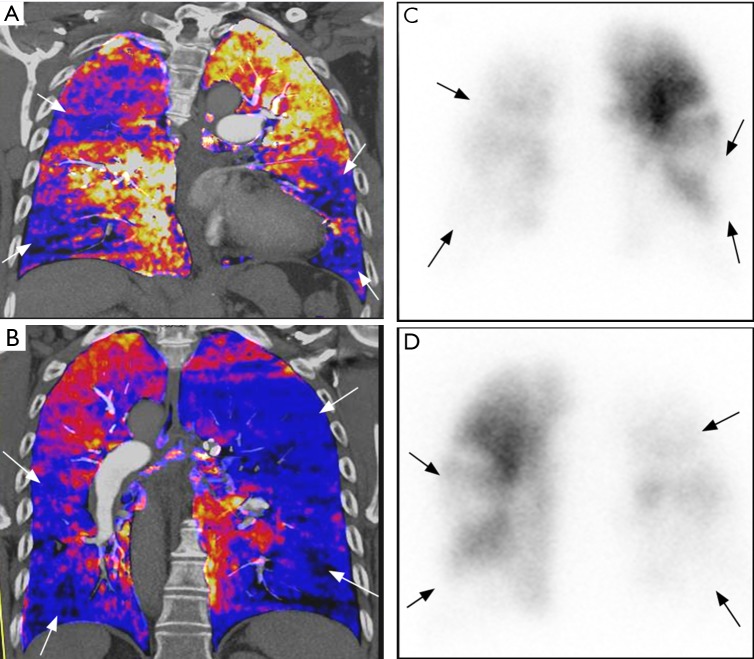
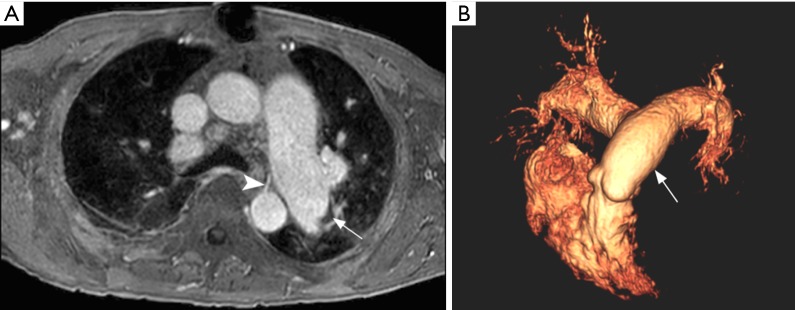
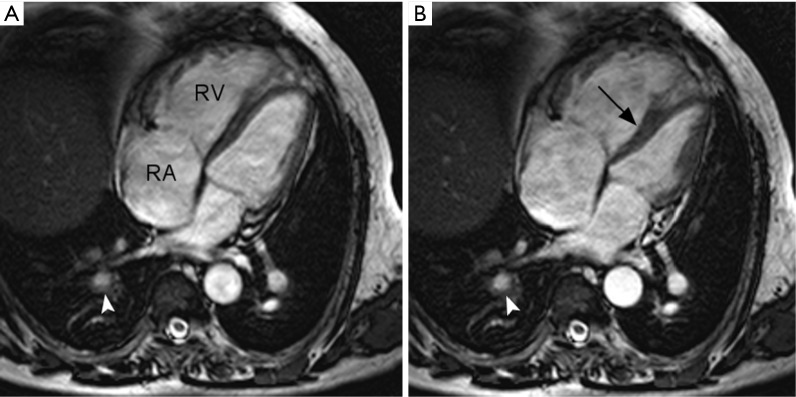
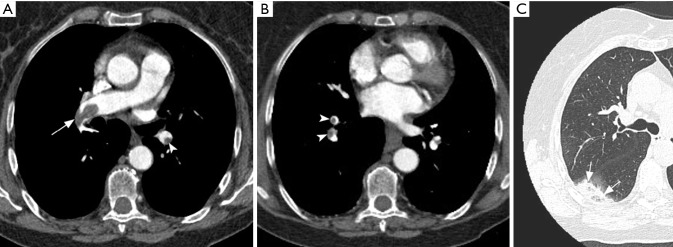
Chronic thromboembolic pulmonary hypertension (CTEPH) is a complication of venous thromboembolic disease. Differently from other causes of pulmonary hypertension, CTEPH is potentially curable with surgery (thromboendarterectomy) or balloon pulmonary angioplasty. Imaging plays a central role in CTEPH diagnosis. The combination of techniques such as lung scintigraphy, computed tomography and magnetic resonance angiography provides non-invasive anatomic and functional information. Conventional pulmonary angiography (CPA) with right heart catheterization (RHC) is considered the gold standard method for diagnosing CTEPH. In this review, we discuss the utility of these imaging techniques in the diagnosis of CTEPH.
Keywords: Pulmonary embolism; V/Q; chronic; computed tomography; pulmonary hypertension.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources