

Radiologic review of acquired pulmonary vein stenosis in adults
- PMID: 30057885
- PMCID: PMC6039802
- DOI: 10.21037/cdt.2018.05.05
Radiologic review of acquired pulmonary vein stenosis in adults
Abstract
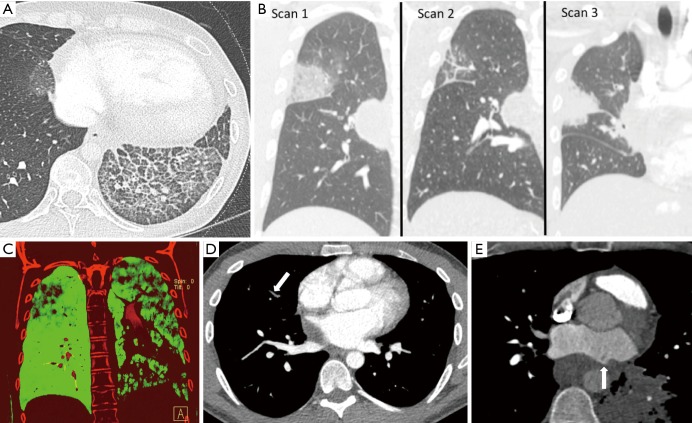
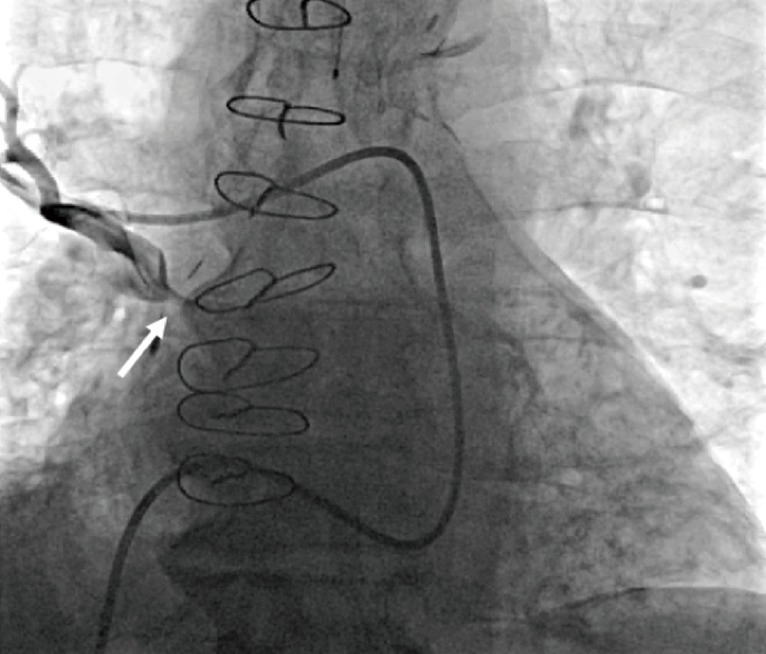
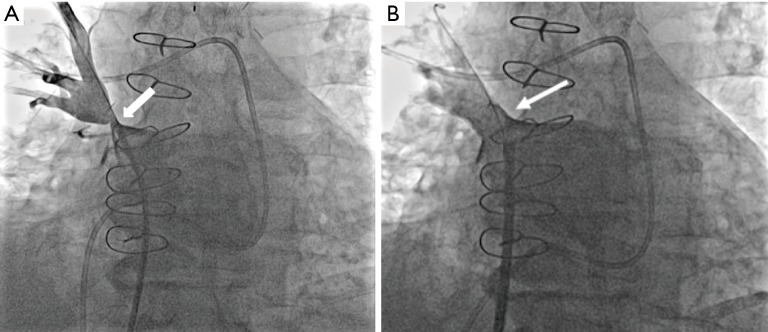
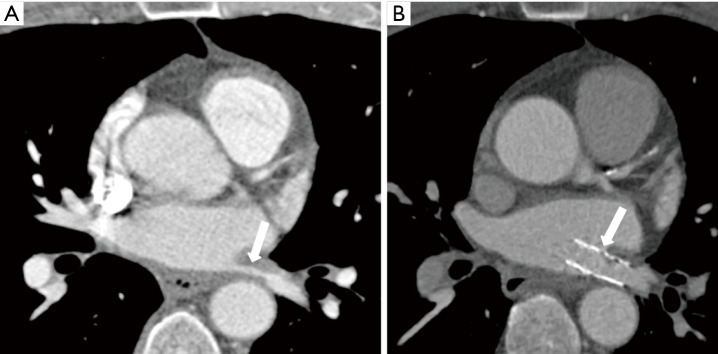
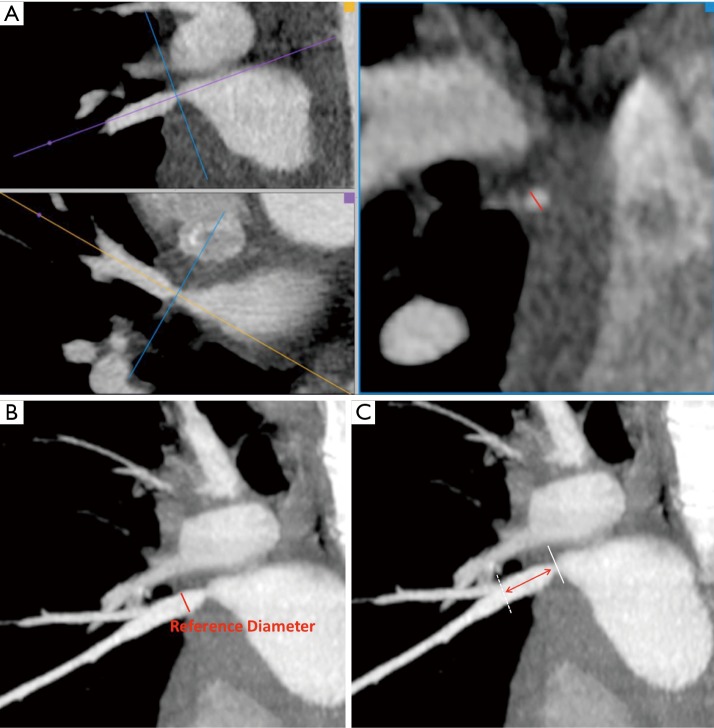
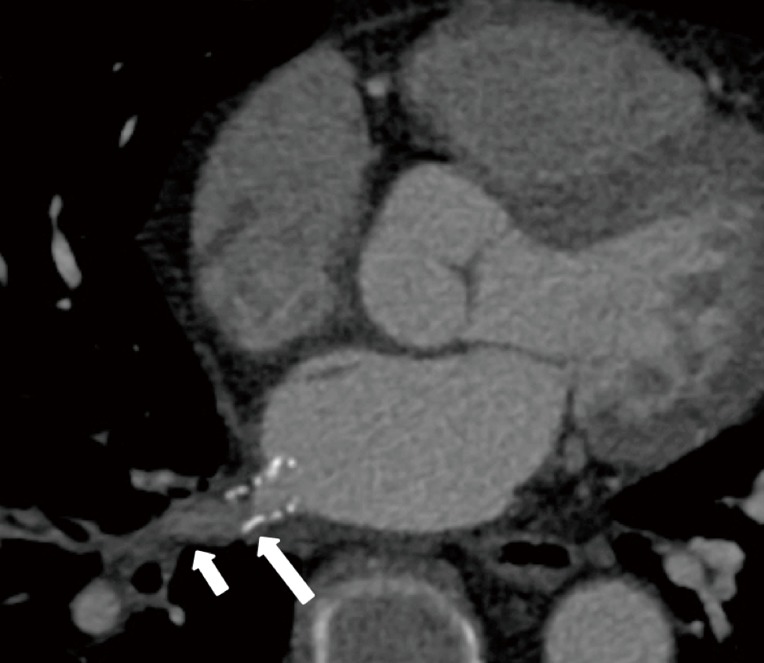
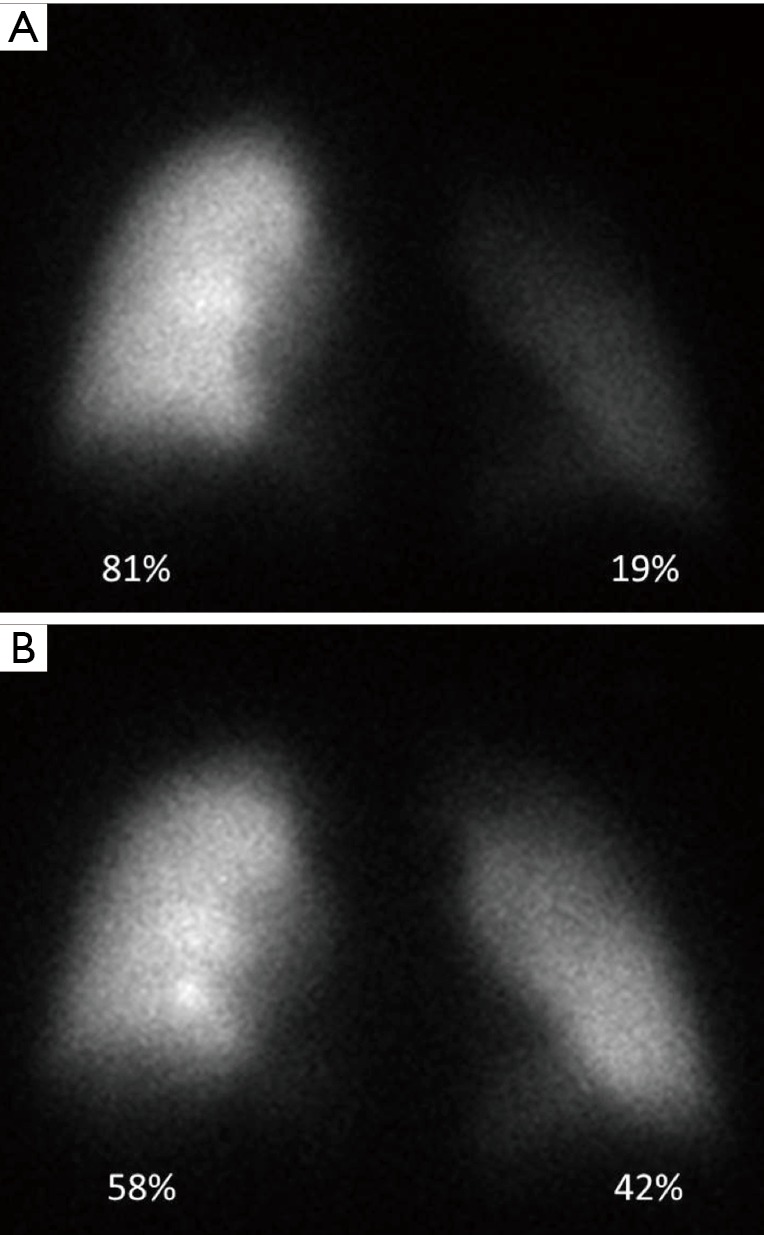
Acquired pulmonary vein stenosis (PVS) is an uncommon occurrence in adults, but one that carries significant morbidity/mortality. PVS can be secondary to neoplastic infiltration/extrinsic compression, non-neoplastic infiltration/extrinsic compression, or iatrogenic intervention. This article: (I) reviews the common causes of acquired PVS; (II) illustrates direct and indirect cross-sectional imaging findings in acquired PVS (in order to avoid misinterpretation of these imaging findings); and (III) details the role of imaging before and after the treatment of acquired PVS.
Keywords: Pulmonary vein stenosis (PVS); computed tomography (CT); imaging; magnetic resonance imaging (MRI); pulmonary vein ablation; pulmonary vein isolation (PVI); radiology.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials