

Comparing the validity of different ICD coding abstraction strategies for sepsis case identification in German claims data
- PMID: 30059504
- PMCID: PMC6066203
- DOI: 10.1371/journal.pone.0198847
Comparing the validity of different ICD coding abstraction strategies for sepsis case identification in German claims data
Abstract
Introduction: Administrative data are used to generate estimates of sepsis epidemiology and can serve as source for quality indicators. Aim was to compare estimates on sepsis incidence and mortality based on different ICD-code abstraction strategies and to assess their validity for sepsis case identification based on a patient sample not pre-selected for presence of sepsis codes.
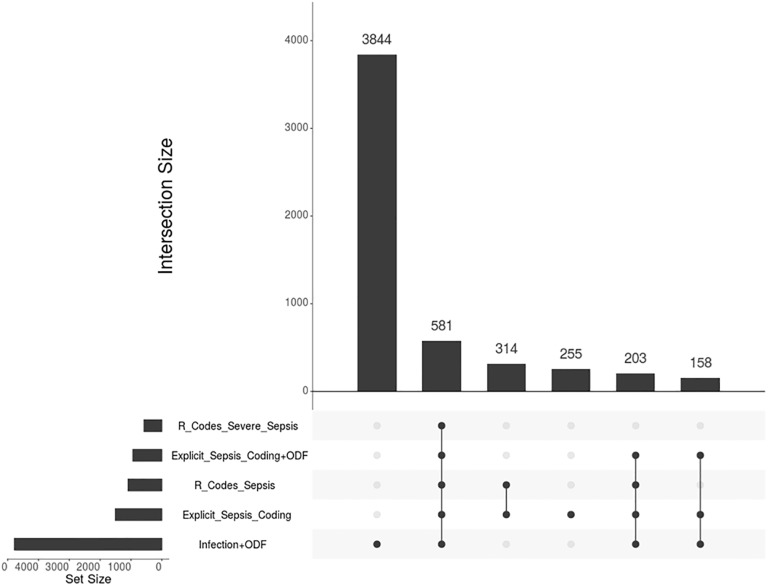
Materials and methods: We used the national DRG-statistics for assessment of population-level sepsis incidence and mortality. Cases were identified by three previously published International Statistical Classification of Diseases (ICD) coding strategies for sepsis based on primary and secondary discharge diagnoses (clinical sepsis codes (R-codes), explicit coding (all sepsis codes) and implicit coding (combined infection and organ dysfunction codes)). For the validation study, a stratified sample of 1120 adult patients admitted to a German academic medical center between 2007-2013 was selected. Administrative diagnoses were compared to a gold standard of clinical sepsis diagnoses based on manual chart review.
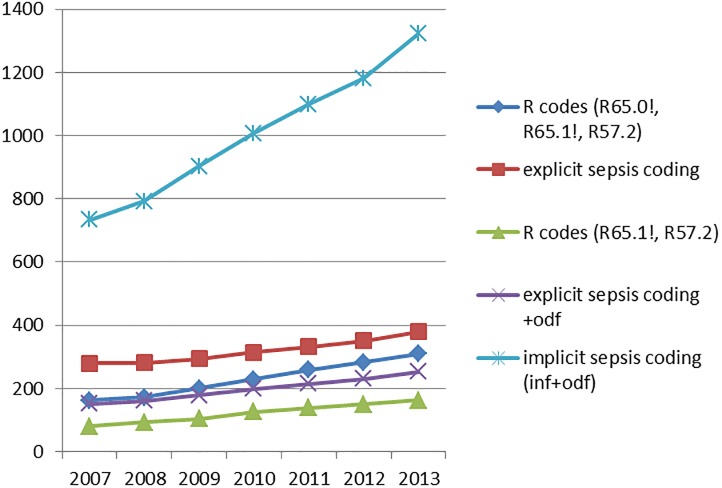
Results: In the validation study, 151/937 patients had sepsis. Explicit coding strategies performed better regarding sensitivity compared to R-codes, but had lower PPV. The implicit approach was the most sensitive for severe sepsis; however, it yielded a considerable number of false positives. R-codes and explicit strategies underestimate sepsis incidence by up to 3.5-fold. Between 2007-2013, national sepsis incidence ranged between 231-1006/100,000 person-years depending on the coding strategy.
Conclusions: In the sample of a large tertiary care hospital, ICD-coding strategies for sepsis differ in their accuracy. Estimates using R-codes are likely to underestimate the true sepsis incidence, whereas implicit coding overestimates sepsis cases. Further multi-center evaluation is needed to gain better understanding on the validity of sepsis coding in Germany.
Conflict of interest statement
The authors have declared that no competing interests exist. The above funding does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Fleischmann C, Scherag A, Adhikari NK, Hartog CS, Tsaganos T, Schlattmann P, et al. Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current Estimates and Limitations. American journal of respiratory and critical care medicine. 2016;193(3):259–72. Epub 2015/09/29. 10.1164/rccm.201504-0781OC . - DOI - PubMed
-
- World Health Organisation Executive Board (EB140/12). Improving the prevention, diagnosis and clinical management of sepsis. 2017 [2017/06/20]. http://apps.who.int/gb/ebwha/pdf_files/EB140/B140_12-en.pdf.
-
- Rhee C, Dantes R, Epstein L, Murphy DJ, Seymour CW, Iwashyna TJ, et al. Estimating The National Burden Of Sepsis Using Clinical Data. American journal of respiratory and critical care medicine. 2017;195:A5010.
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Critical care medicine. 2001;29(7):1303–10. Epub 2001/07/11. . - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
