

Failure to Launch: Targeting Inflammation in Acute Coronary Syndromes
- PMID: 30062164
- PMCID: PMC6034453
- DOI: 10.1016/j.jacbts.2017.07.001
Failure to Launch: Targeting Inflammation in Acute Coronary Syndromes
Abstract
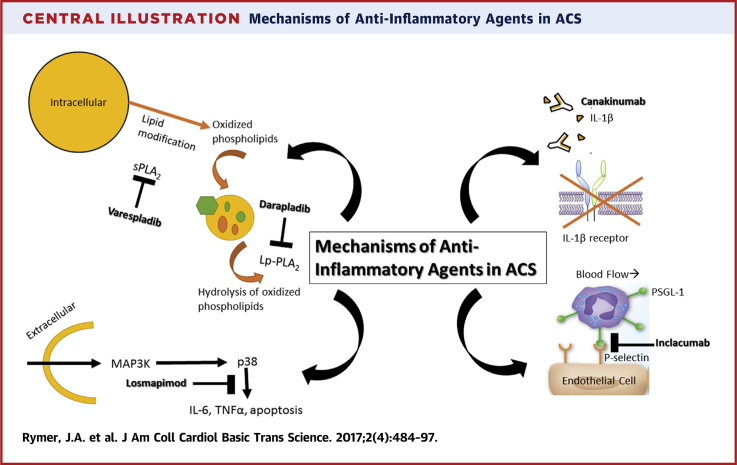
The importance of inflammation and inflammatory pathways in atherosclerotic disease and acute coronary syndromes (ACS) is well established. The success of statin therapy rests not only on potently reducing levels of low-density lipoprotein cholesterol, but also on the many beneficial, pleiotropic effects statin therapy has on various inflammatory mechanisms in atherosclerotic disease, from reducing endothelial dysfunction to attenuating levels of serum C-reactive protein. Due to the growing awareness of the importance of inflammation in ACS, investigators have attempted to develop novel therapies against known markers of inflammation for several decades. Targeted pathways have ranged from inhibiting C5 cleavage with a high-affinity monoclonal antibody against C5 to inhibiting the activation of the p38 mitogen-activated protein kinase signaling cascades. In each of these instances, despite promising early preclinical and mechanistic studies and phase 2 trials suggesting a potential benefit in reducing post-MI complications or restenosis, these novel therapies have failed to show benefits during large, phase 3 clinical outcomes trials. This review discusses several examples of novel anti-inflammatory therapies that failed to show significant improvement on clinical outcomes when tested in large, randomized trials and highlights potential explanations for why targeted therapies against known markers of inflammation in ACS have failed to launch.
Keywords: ACS, acute coronary syndromes; CABG, coronary artery bypass graft; CAD, coronary artery disease; HDL-C, high-density lipoprotein cholesterol; IL, interleukin; LDL-C, low-density lipoprotein cholesterol; Lp-PLA2, lipoprotein-associated phospholipase A2; MAPK, mitogen-activated protein kinase; MI, myocardial infarction; NSTEMI, non–ST-segment myocardial infarction; PCI, percutaneous coronary intervention; PSGL, P-selectin glycoprotein ligand; STEMI, ST-segment elevation myocardial infarction; SVG, saphenous vein grafts; TBR, tissue-to-background ratio; acute coronary syndrome; anti-inflammatory; drug targets; hsCRP, high-sensitivity C-reactive protein; sPLA2, secretory phospholipase A2.
Figures



References
-
- Yeh R.W., Sidney S., Chandra M., Sorel M., Selby J.V., Go A.S. Population trends in the incidence and outcomes of acute myocardial infarction. N Engl J Med. 2010;362:2155–2165. - PubMed
-
- Tobbia P., Brodie B.R., Witzenbichler B. Adverse event rates following primary PCI for STEMI at US and non-US hospitals: three-year analysis from the HORIZONS-AMI trial. EuroIntervention. 2013;8:1134–1142. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
