

Improving perfusion defect detection with respiratory motion correction in cardiac SPECT at standard and reduced doses
- PMID: 30062470
- PMCID: PMC11380466
- DOI: 10.1007/s12350-018-1374-9
Improving perfusion defect detection with respiratory motion correction in cardiac SPECT at standard and reduced doses
Abstract
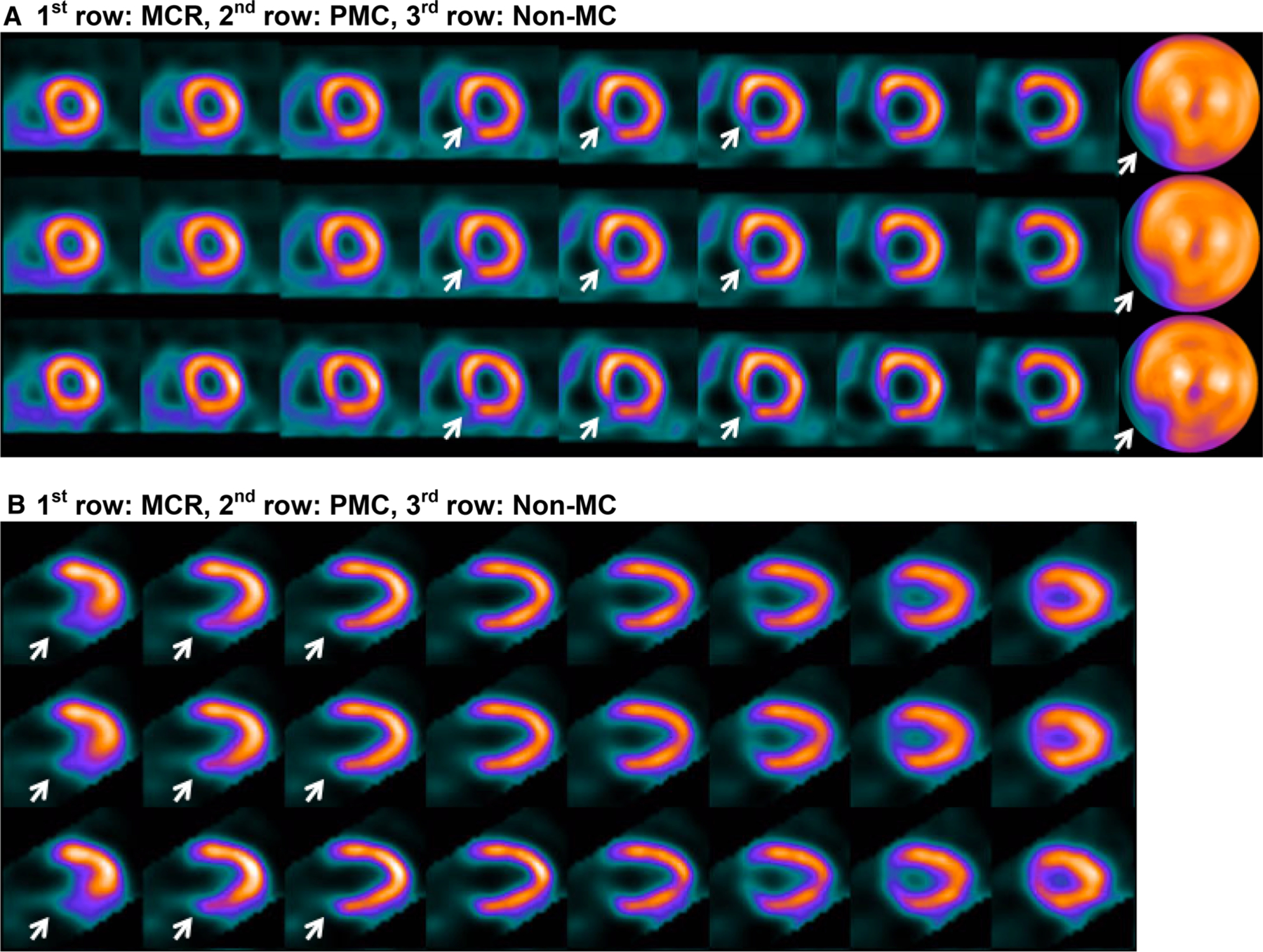
Background: In cardiac SPECT perfusion imaging, respiratory motion can cause non-uniform blurring in the reconstructed myocardium. We investigate the potential benefit of respiratory correction with respiratory-binned acquisitions, both at standard dose and at reduced dose, for defect detection and for left ventricular (LV) wall resolution.
Methods: We applied two reconstruction methods for respiratory motion correction: post-reconstruction motion correction (PMC) and motion-compensated reconstruction (MCR), and compared with reconstruction without motion correction (Non-MC). We quantified the presence of perfusion defects in reconstructed images by using the total perfusion deficit (TPD) scores and conducted receiver-operating-characteristic (ROC) studies using TPD. We quantified the LV spatial resolution by using the FWHM of its cross-sectional intensity profile.
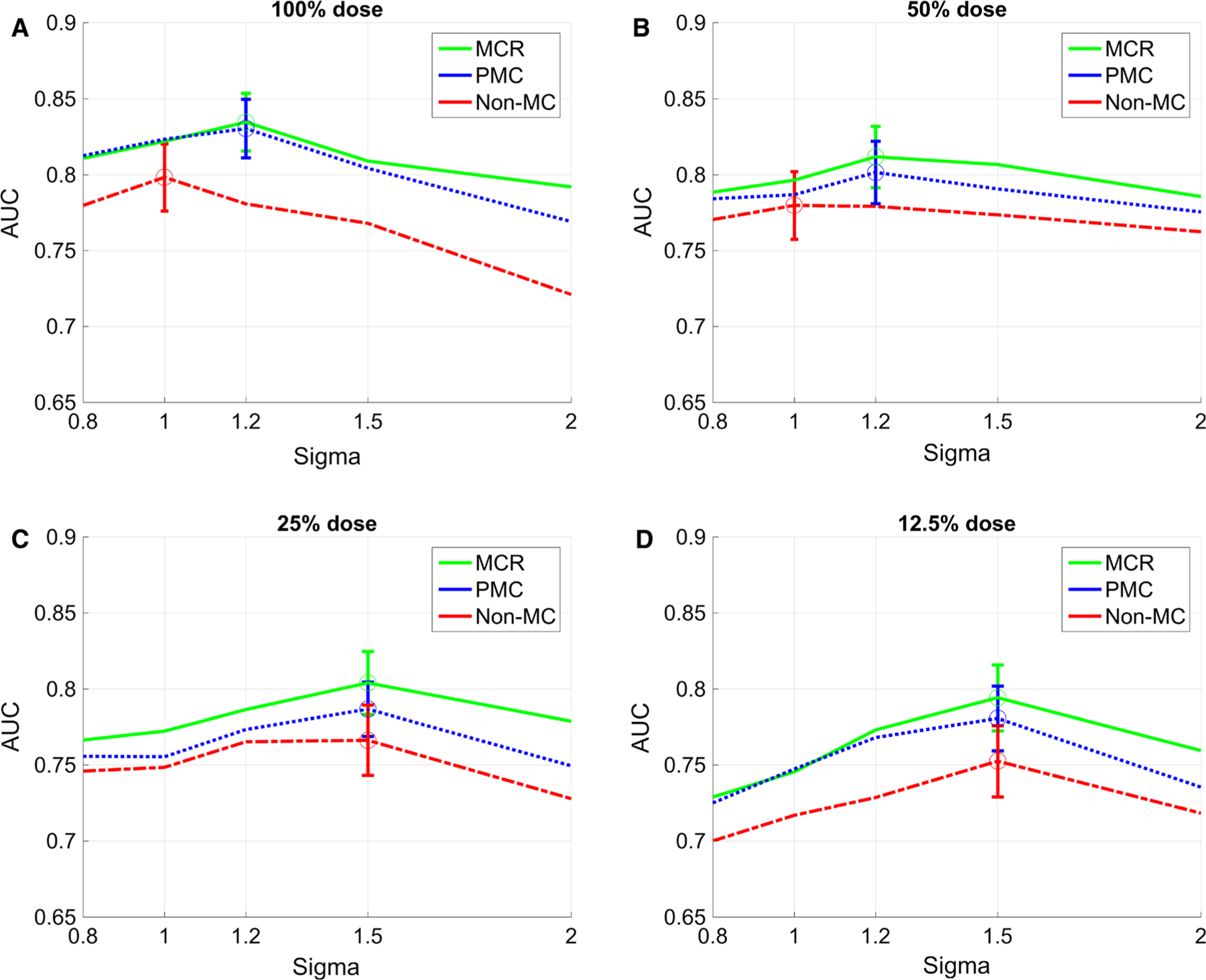
Results: The values in the area-under-the-ROC-curve (AUC) achieved by MCR, PMC, and Non-MC at standard dose were 0.835, 0.830, and 0.798, respectively. Similar AUC improvements were also obtained by MCR and PMC over Non-MC at 50%, 25%, and 12.5% of full dose. Improvements in LV resolution were also observed with motion correction.
Conclusions: Respiratory-binned acquisitions can improve perfusion-defect detection accuracy over traditional reconstruction both at standard dose and at reduced dose. Motion correction may contribute to achieving further dose reduction while maintaining the diagnostic accuracy of traditional acquisitions.
Antecedentes.: En los estudios de perfusión cardiaca por SPECT, los movimientos respiratorios pueden causar distorsión no uniforme en el miocardio reconstruido. Investigamos el beneficio potencial de la corrección respiratoria con adquisición de imágenes sincronizadas con la respiración, tanto a dosis estándar como a dosis reducida, para detección de defectos y para resolución de pared de ventrículo izquierdo (VI).
Métodos.: Aplicamos dos métodos de reconstrucción para corrección de movimientos respiratorios: Corrección de movimiento post reconstrucción (PMC) y reconstrucción compensada a movimiento (MCR), y los comparamos con la reconstrucción sin corrección de movimiento (Non-MC). Cuantificamos la presencia de defectos de perfusión en las imágenes reconstruidas usando los scores de déficit total de perfusión (TPD) y análisis ROC usando el TPD. Cuantificamos la resolución espacial del VI usando la anchura a media altura de su perfil de intensidad transversal.
Resultados.: Los valores en el área bajo la curva ROC (ABC) obtenidos por MCR, PMC y Non-MC a dosis estándar fueron 0.835, 0.830 y 0.798, respectivamente. Mejorías similares del ABC también se obtuvieron por MCR y PMC, sobre Non-MC a 50%, 25% y 12.5% de la dosis completa. Las mejorías en la resolución del VI fueron observadas también con corrección del movimiento.
Conclusiones.: Las adquisiciones sincronizadas con la respiración pueden mejorar la precisión de la detección de defectos de perfusión sobre las reconstrucciones tradicionales tanto a dosis estándar como a dosis reducida. La corrección de movimiento puede contribuir a lograr mayor reducción de la dosis manteniendo la precisión diagnóstica de las adquisiciones tradicionales.
背景.: 在心脏 SPECT 灌注成像中, 呼吸运动会导致心肌重建的不均匀模糊。我们研究了无论是标准剂量还是减少剂量的情况下, 呼吸跟踪采集的呼吸校正用于图像缺损检测和左心室(LV) 室壁分辨率的潜在益处。
方法.: 我们使用了两种呼吸运动校正的重建方法:重建后运动校正 (PMC) 和运动补偿重建(MCR), 并与没有运动校正的重建(Non-MC) 进行比较。 通过总灌注缺损(TPD) 评分和其接受者操作特性曲线 (ROC) 来量化重建图像中的灌注缺陷。通过LV横截面强度分布的 FWHM来量化 LV 空间分辨率。
结果.: MCR, PMC 和 Non-MC 在标准剂量下所获得的 ROC 曲线下面积 (AUC) 的值分别为0.835, 0.830 和 0.798。 在全剂量下, MCR, PMC和Non-MC 也获得类似的AUC 提高,分别为50%, 25% 和 12.5%。 在运动校正下, LV的分辨率也得到了改善。
结论.: 在标准剂量和减少剂量的情况下,呼吸跟踪采集可以改善灌注缺损检测的准确性。运动校正可能有助于进一步实现减少剂量的目标, 同时保证通过传统检测方法的诊断准确性。
Contexte.: Les mouvements respiratoires peuvent entrainer des artefacts de uniformité lors de la reconstruction des images de perfusion myocardique en SPECT. Dans cet article, nous rapportons nos résultats sur le bénéfice potentiel du « gating » respiratoire avec des doses standards et réduites de radio-pharmaceutiques pour la détection des anomalies de perfusion et les mesures de la paroi ventriculaire gauche.
Méthodes.: Nous avons appliqué deux méthodes de reconstruction pour la correction du mouvement respiratoire: la première fait appel a une correction après reconstruction des images (PMC) ; la seconde fait appel à la correction des images avant reconstruction (MRC). Les deux approches ont été comparées à la reconstruction sans correction de mouvement (Non-MC). Nous avons quantifié les déficits de perfusion myocardiques sur les images reconstruites avec le système des scores de déficit de perfusion et analysé les résultats en utilisant les courbes ROC. Nous avons quantifié la résolution spatiale du VG en utilisant le FWHM du profil d’intensité de sa section transversale.
Résultats.: Les valeurs des surfaces en dessous des courbes ROC (AUC) obtenues par MCR, PMC et Non-MC avec doses standard de radio-pharmaceutiques étaient de 0,835, 0,830 et 0,798, respectivement. Des améliorations similaires de l’AUC ont également été obtenues par MCR et PMC sur Non-MC avec 50%, 25% et 12,5% des doses entières. Les mesures de resolution spatiale de la paroi du VG ont également été améliorées avec la correction des mouvements respiratoires.
Conclusions.: La correction des images de perfusion myocardiques en SPECT par « gating » respiratoire paraît améliorer la quantification des déficits perfusionels à la fois à dose standard et à dose réduite de radio-pharmaceutiques. L’application de cette correction devrait permettre de réduire les doses de radio-pharmaceutiques utilisées tout en maintenant la précision diagnostique des acquisitions traditionnelles.
Keywords: CAD; MPI; SPECT; image reconstruction.
Figures





References
-
- DePuey EG. Garcia. Updated imaging guidelines for nuclear cardiology procedures part I. J Nucl Cardiol 2001;8:G5–58. - PubMed
-
- Lin GS, Hines HH, Grant G, Taylor K, Ryals C. Automated quantification of myocardial ischemia and wall motion defects by use of cardiac SPECT polar mapping and 4-dimensional surface rendering. J Nucl Med Technol 2006;34:3–17. - PubMed
-
- Arsanjani R, Xu Y, Hayes SW, Fish M, Lemley M, Gerlach J, Dorbala S, Berman DS, Germano G, Slomka P. Comparison of fully automated computer analysis and visual scoring for detection of coronary artery disease from myocardial perfusion SPECT in a large population. J Nucl Med 2013;54:221–8. - PMC - PubMed
-
- Slomka PJ, Nishina H, Berman DS, Akincioglu C, Abidov A, Friedman JD, Hayes SW, Germano G. Automated quantification of myocardium perfusion SPECT using simplified normal limits. J Nucl Cardiol 2005;12:66–77. - PubMed
-
- Cooper JA, Neumann PH, McCandless BK. Effect of patient motion on tomographic myocardial perfusion imaging. J Nucl Med 1992;33:1566–71. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
