

Cross-sectional validation of the PROMIS-Preference scoring system
- PMID: 30063733
- PMCID: PMC6067708
- DOI: 10.1371/journal.pone.0201093
Cross-sectional validation of the PROMIS-Preference scoring system
Abstract
Objectives: The PROMIS-Preference (PROPr) score is a recently developed summary score for the Patient-Reported Outcomes Measurement Information System (PROMIS). PROPr is a preference-based scoring system for seven PROMIS domains created using multiplicative multi-attribute utility theory. It serves as a generic, societal, preference-based summary scoring system of health-related quality of life. This manuscript evaluates construct validity of PROPr in two large samples from the US general population.
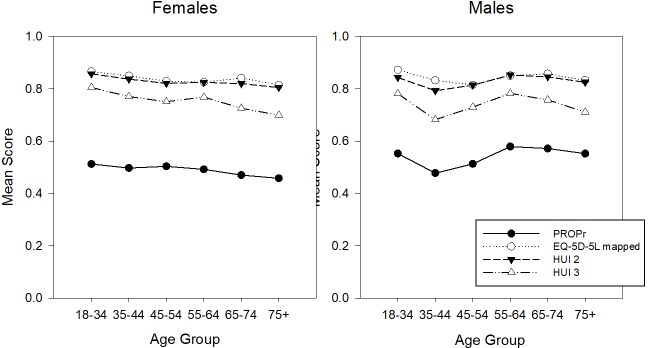
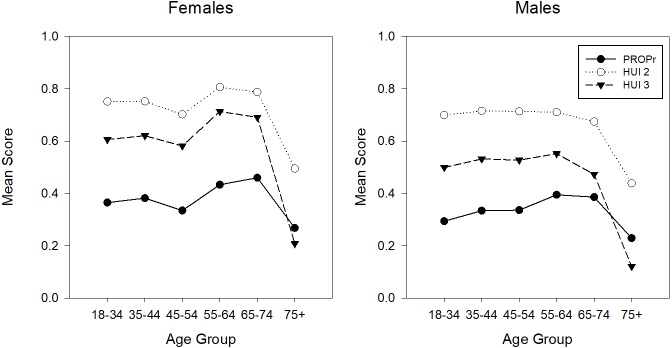
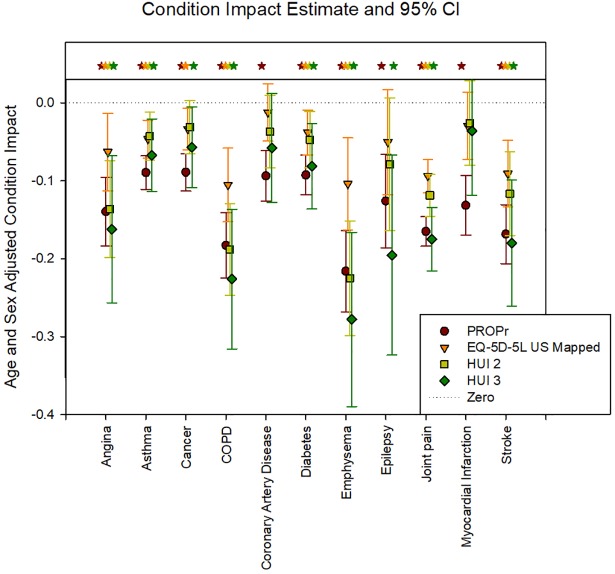
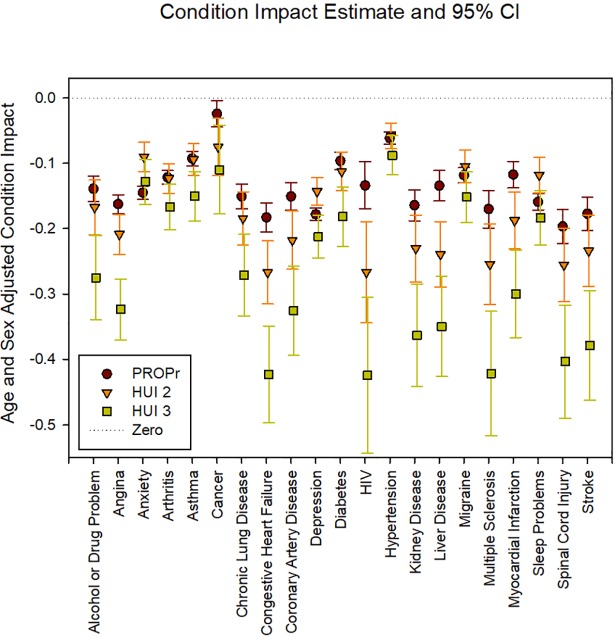
Methods: We utilized 2 online panel surveys, the PROPr Estimation Survey and the Profiles-Health Utilities Index (HUI) Survey. Both included the PROPr measure, patient demographic information, self-reported chronic conditions, and other preference-based summary scores: the EuroQol-5D (EQ-5D-5L) and HUI in the PROPr Estimation Survey and the HUI in the Profiles-HUI Survey. The HUI was scored as both the Mark 2 and the Mark 3. Known-groups validity was evaluated using age- and gender-stratified mean scores and health condition impact estimates. Condition impact estimates were created using ordinary least squares regression in which a summary score was regressed on age, gender, and a single health condition. The coefficient for the health condition is the estimated effect on the preference score of having a condition vs. not having it. Convergent validity was evaluated using Pearson correlations between PROPr and other summary scores.
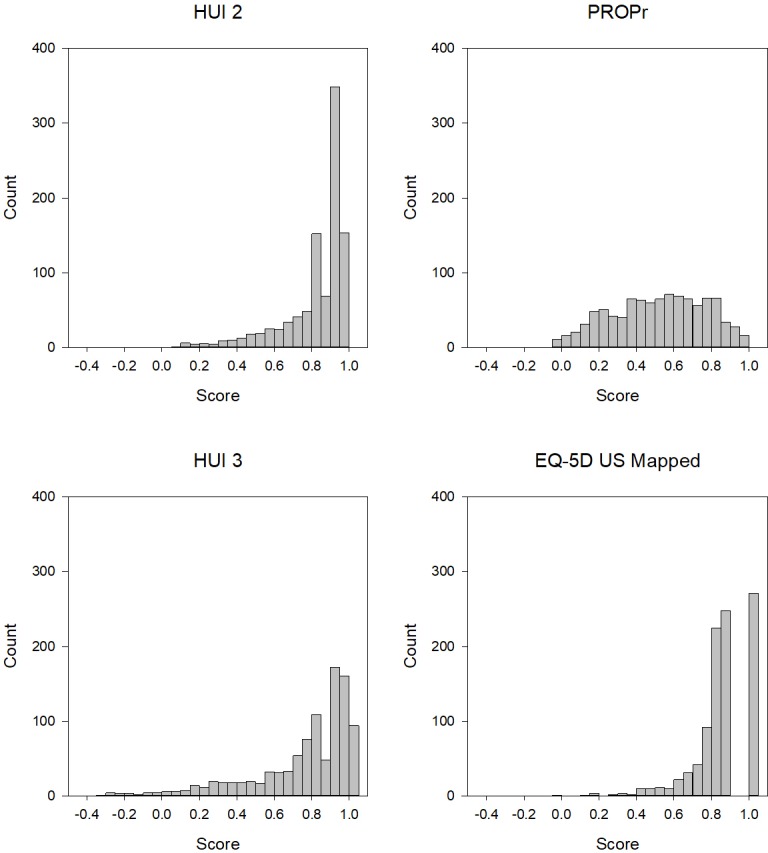
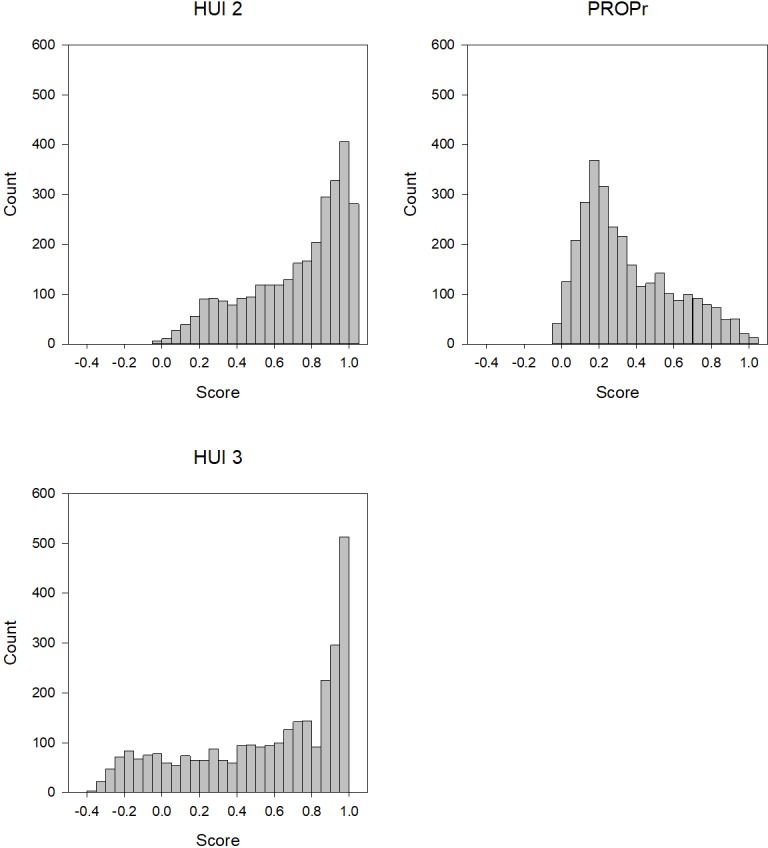
Results: The sample consisted of 983 respondents from the PROPr Estimation Survey and 3,000 from the Profiles-HUI survey. Age- and gender-stratified mean PROPr scores were lower than EQ-5D and HUI scores, with fewer subjects having scores corresponding to perfect health on the PROPr. In the PROPr Estimation survey, all 11 condition impact estimates were statistically significant using PROPr, 8 were statistically significant by the EQ-5D, 7 were statistically significant by HUI Mark 2, and 9 were statistically significant by HUI Mark 3. In the Profiles-HUI survey, all 21 condition impact estimates were statistically significant using summary scores from all three scoring systems. In these samples, the correlations between PROPr and the other summary measures ranged from 0.67 to 0.70.
Conclusions: These results provide evidence of construct validity for PROPr using samples from the US general population.
Conflict of interest statement
David Feeny has a proprietary interest in Health Utilities Incorporated, Dundas, Ontario, Canada. HUInc. distributes copyrighted Health Utilities Index (HUI) materials and provides methodological advice on the use of the HUI. Dennis Revicki is employed by Evidera, Inc. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- McHorney CA. Health status assessment methods for adults: past accomplishments and future challenges. Annual review of public health. 1999. May;20(1):309–35. - PubMed
-
- Wilson IB, Cleary PD. Linking clinical variables with health-related quality of life: a conceptual model of patient outcomes. Jama. 1995. January 4;273(1):59–65. - PubMed
-
- McDowell I. Measuring health: a guide to rating scales and questionnaires. Oxford university press; 2006. March 9.
-
- Tengs TO, Wallace A. One thousand health-related quality-of-life estimates. Medical care. 2000. June 1:583–637. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
