

Assessment of changes of regional ventilation distribution in the lung tissue depending on the driving pressure applied during high frequency jet ventilation
- PMID: 30064377
- PMCID: PMC6069840
- DOI: 10.1186/s12871-018-0552-2
Assessment of changes of regional ventilation distribution in the lung tissue depending on the driving pressure applied during high frequency jet ventilation
Abstract
Background: Electrical impedance tomography (EIT) is a tool to monitor regional ventilation distribution in patient's lungs under general anesthesia. The objective of this study was to assess the regional ventilation distribution using different driving pressures (DP) during high frequency jet ventilation (HFJV).
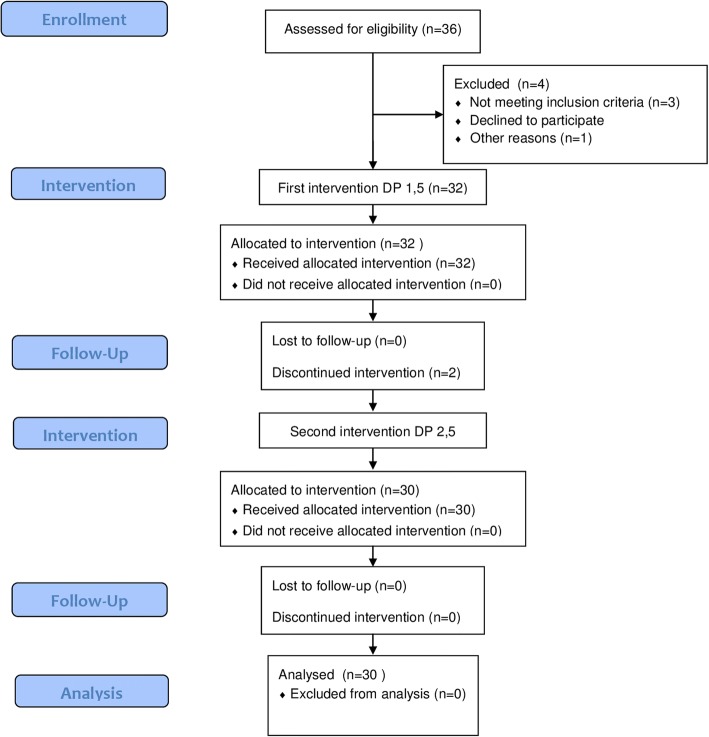
Methods: Prospective, observational, cross-over study. Patients undergoing rigid bronchoscopy were ventilated HFJV with DP 1.5 and 2.5 atm. Hemodynamic and ventilation parameters, as well as ventilation in different regions of the lungs in percentage of total ventilation, assessed by EIT, were recorded.
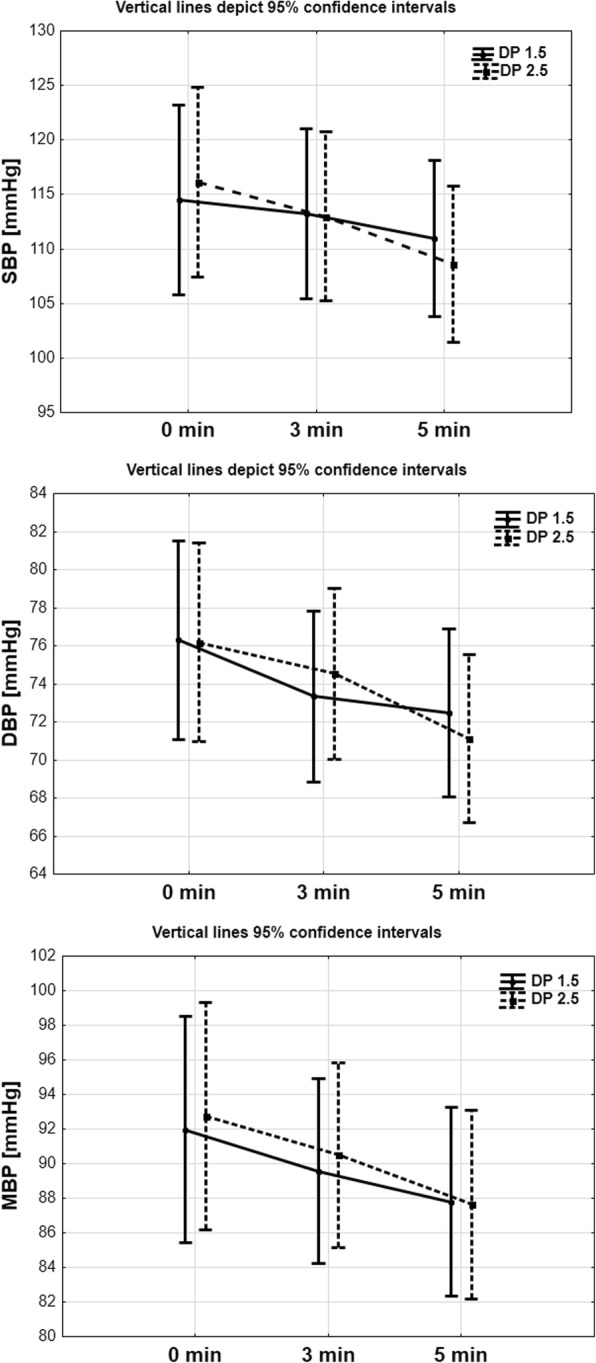
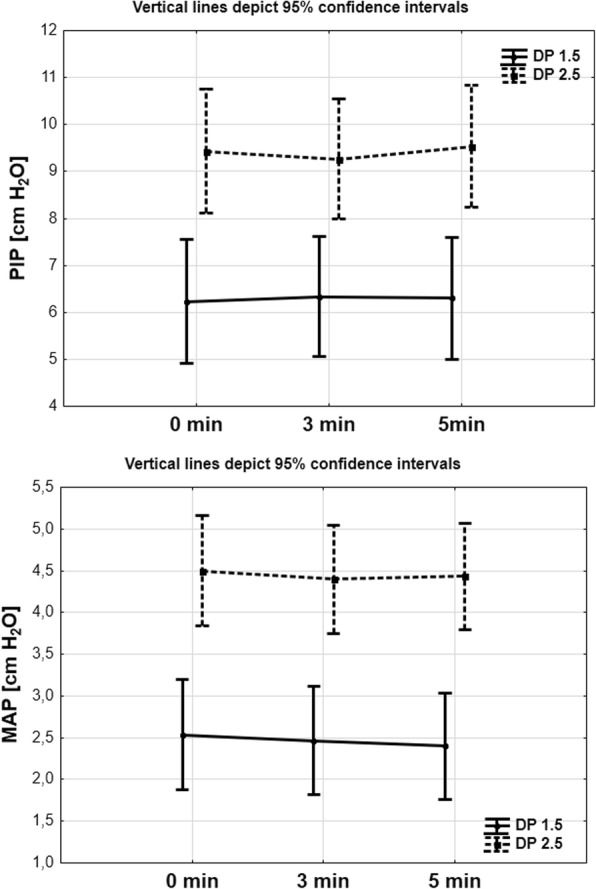
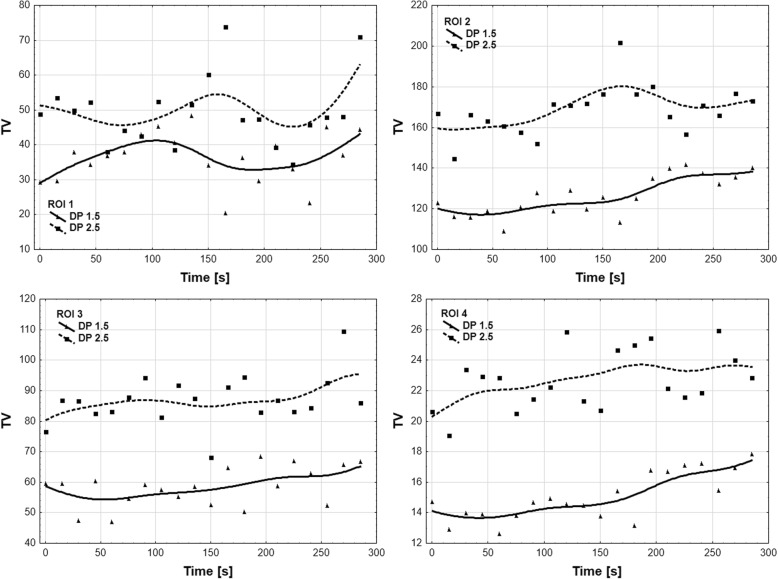
Results: Thirty-six patients scheduled for elective rigid bronchoscopy. The final analysis included thirty patients. There was no significant difference in systolic, diastolic and mean arterial blood pressure, heart rate, and peripheral saturation between the two groups. Peak inspiratory pressure, mean inspiratory pressure, tidal volume, and minute volume significantly increased in the second, compared to the first intervention group. Furthermore, there were no statistically significant differences between each time profiles in all ROI regions in EIT.
Conclusions: In our study intraoperative EIT was an effective method of functional monitoring of the lungs during HFJV for rigid bronchoscopy procedure. Lower driving pressure was as effective in providing sufficient ventilation distribution through the lungs as the higher driving pressure but characterized by lower airway pressure.
Trial registration: The study was registered on ClinicalTrials.gov under no. NCT02997072 .
Keywords: Driving pressure; High frequency; Inspiratory pressure; Jet ventilation.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol has been approved by the Institutional Review Boards of the Medical University of Silesia, Katowice, Poland (identifier: KNW/0022/KB1/42/16), and written informed consent was obtained from the patients before their enrollment in the study.
Consent for publication
All included patients or their family members signed the informed consent form to report individual patient data. All authors have confirmed the manuscript and approved the publication of the manuscript.
Competing interests
Kurt Ruetzler, MD serves as an associate editor of BMC Anesthesiology, but was not involved in handling this manuscript in any manner. The authors declare that they have no competing interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
