

Physiotherapy plus conventional treatment versus conventional treatment only in the treatment of functional constipation in children: design of a randomized controlled trial and cost-effectiveness study in primary care
- PMID: 30064408
- PMCID: PMC6069950
- DOI: 10.1186/s12887-018-1231-7
Physiotherapy plus conventional treatment versus conventional treatment only in the treatment of functional constipation in children: design of a randomized controlled trial and cost-effectiveness study in primary care
Abstract
Background: Our aim was to design a study to evaluate the effectiveness and cost-effectiveness of adding physiotherapy to conventional treatment for children with functional constipation in primary care. Physiotherapy is focusing on improving the coordination between the pelvic floor and abdominal musculature during bowel movement, while conventional treatment is mainly focusing on symptomatic relief of symptoms, therefore, we expect the effects of physiotherapy will be more sustainable than the effects of conventional treatment. In this paper we describe the final study design and how the design was adapted, to overcome recruitment problems.
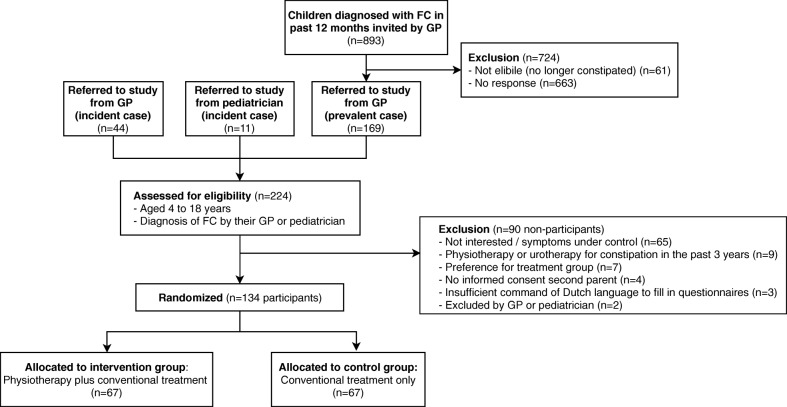
Methods: We designed a randomized controlled trial of children aged 4-17 years with functional constipation diagnosed by a general practitioner or pediatrician. Children in the intervention group received physiotherapy plus conventional treatment, and those in the control group received conventional treatment only. Follow-up measurements took place at 4 and 8 months. The primary outcome was treatment success defined according to the Rome-III criteria as the absence of functional constipation, with no laxative use. Secondary outcomes were absence of functional constipation irrespective of laxative use, quality of life, global perceived effect, and costs. Children were recruited from September 2014 to February 2017. Initially, we aimed to include children with recent symptom onset. However, in the first phase of enrollment we were confronted with an unforeseen recruitment problem: many children and their parents refused randomization because physiotherapy was considered too burdensome for the stage of disease. Therefore, we decided to also include children with a longer duration of symptoms. In total 134 children were included.
Discussion: The target number of participants is achieved. Therefore, the results may change thinking about the management of functional constipation in children.
Trail registration: Netherlands Trial Register ( NTR4797 ), registered 8 September 2014.
Keywords: Child and adolescent; Constipation; Family medicine; General practitioner; Pelvic floor.
Conflict of interest statement
Ethics approval and consent to participate
The trial was approved by the Medical Ethical Board of the University Medical Center of Groningen (METC2013/331). We obtained informed consent from both the parent(s) and the child (if aged ≥12 years) before enrollment.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Nederlandse Vereniging voor Kindergeneeskunde, Nederlands Huisarts Genootschap: Richtlijn obstipatie bij kinderen van 0 tot 18 jaar. 2009. http://www.nvk.nl/Portals/0/richtlijnen/Obstipatie/Obstipatie%20bij%20ki...
-
- National Collaborating Centre for Women’s and Children’s Health (UK) Constipation in children and youn people: diagnosis and management of idiopathic childhood constipation in primary and secondary care. 2010. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
